

Impaired contractility and remodeling of the upper gastrointestinal tract in diabetes mellitus type-1
- PMID: 17828820
- PMCID: PMC4611767
- DOI: 10.3748/wjg.v13.i36.4881
Impaired contractility and remodeling of the upper gastrointestinal tract in diabetes mellitus type-1
Abstract
Aim: To investigate that both the neuronal function of the contractile system and structural apparatus of the gastrointestinal tract are affected in patients with longstanding diabetes and auto mic neuropathy.
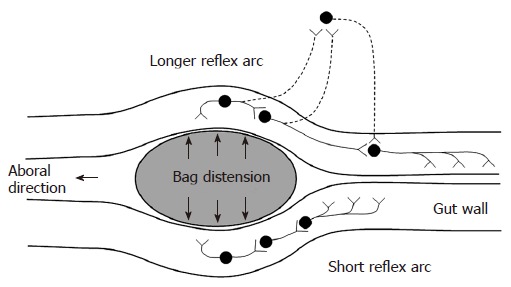
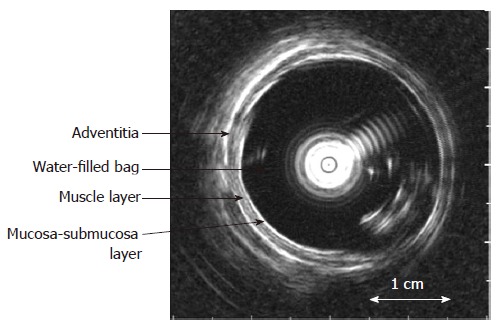
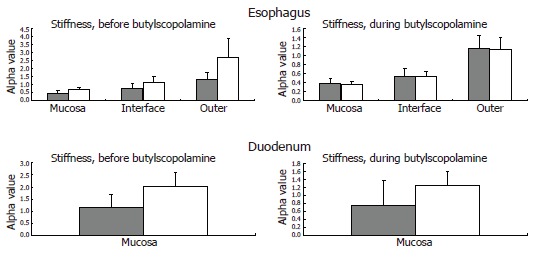
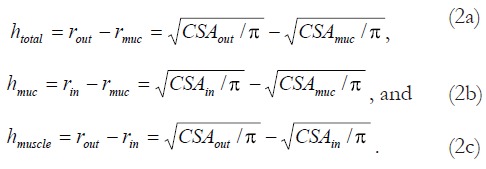
Methods: The evoked esophageal and duodenal contractile activity to standardized bag distension was assessed using a specialized ultrasound-based probe. Twelve type-1 diabetic patients with autonomic neuropathy and severe gastrointestinal symptoms and 12 healthy controls were studied. The geometry and biomechanical parameters (strain, tension/stress, and stiffness) were assessed.
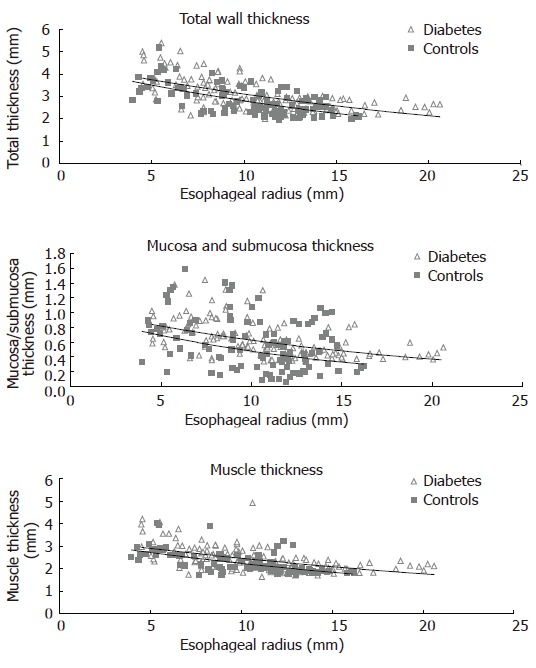
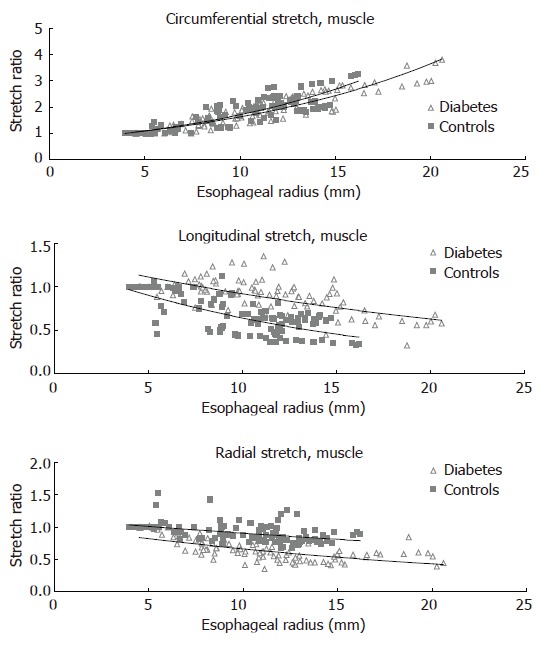
Results: The diabetic patients had increased frequency of distension-induced contractions (6.0 +/- 0.6 vs 3.3 +/- 0.5, P < 0.001). This increased reactivity was correlated with the duration of the disease (P = 0.009). Impaired coordination of the contractile activity in diabetic patients was demonstrated as imbalance between the time required to evoke the first contraction at the distension site and proximal to it (1.5 +/- 0.6 vs 0.5 +/- 0.1, P = 0.03). The esophageal wall and especially the mucosa-submucosa layer had increased thickness in the patients (P < 0.001), and the longitudinal and radial compressive stretch was less in diabetics (P < 0.001). The esophageal and duodenal wall stiffness and circumferential deformation induced by the distensions were not affected in the patients (all P > 0.14).
Conclusion: The impaired contractile activity with an imbalance in the distension-induced contractions likely reflects neuronal abnormalities due to autonomic neuropathy. However, structural changes and remodeling of the gastrointestinal tract are also evident and may add to the neuronal changes. This may contribute to the pathophysiology of diabetic gut dysfunction and impact on future management of diabetic patients with gastrointestinal symptoms.
Figures






References
-
- Rundles RW. Diabetic Neuropathy. Medicine. 1945;24:111–160.
-
- Ko GT, Chan WB, Chan JC, Tsang LW, Cockram CS. Gastrointestinal symptoms in Chinese patients with Type 2 diabetes mellitus. Diabet Med. 1999;16:670–674. - PubMed
-
- Folwaczny C, Riepl R, Tschöp M, Landgraf R. Gastrointestinal involvement in patients with diabetes mellitus: Part I (first of two parts). Epidemiology, pathophysiology, clinical findings. Z Gastroenterol. 1999;37:803–815. - PubMed
-
- Spångéus A, El-Salhy M, Suhr O, Eriksson J, Lithner F. Prevalence of gastrointestinal symptoms in young and middle-aged diabetic patients. Scand J Gastroenterol. 1999;34:1196–1202. - PubMed
-
- Horowitz M, Samsom M. Gastrointestinal Function in Diabetes Mellius. Chichester: John Wiley & Sons Ltd; 2004. pp. 1–27.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
