

Exercise and pharmacotherapy in the treatment of major depressive disorder
- PMID: 17846259
- PMCID: PMC2702700
- DOI: 10.1097/PSY.0b013e318148c19a
Exercise and pharmacotherapy in the treatment of major depressive disorder
Abstract
Objective: To assess whether patients receiving aerobic exercise training performed either at home or in a supervised group setting achieve reductions in depression comparable to standard antidepressant medication (sertraline) and greater reductions in depression compared to placebo controls.
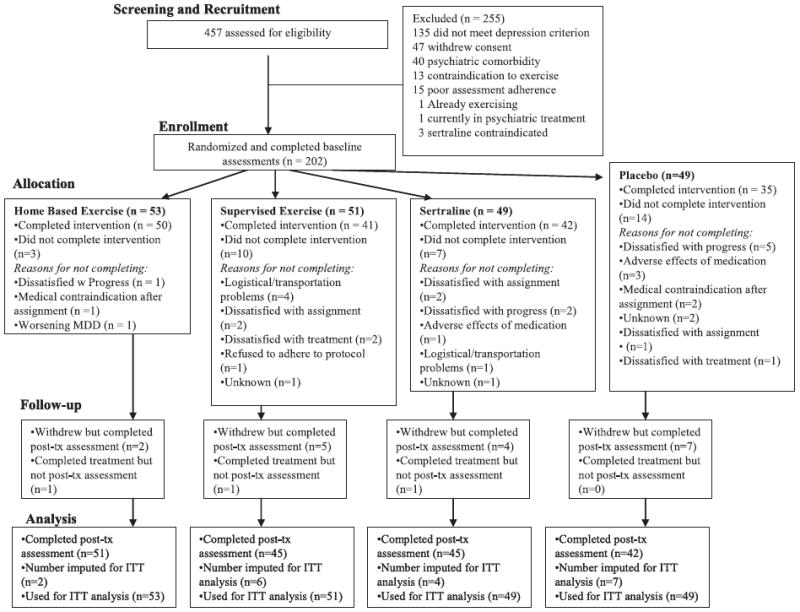
Methods: Between October 2000 and November 2005, we performed a prospective, randomized controlled trial (SMILE study) with allocation concealment and blinded outcome assessment in a tertiary care teaching hospital. A total of 202 adults (153 women; 49 men) diagnosed with major depression were assigned randomly to one of four conditions: supervised exercise in a group setting; home-based exercise; antidepressant medication (sertraline, 50-200 mg daily); or placebo pill for 16 weeks. Patients underwent the structured clinical interview for depression and completed the Hamilton Depression Rating Scale (HAM-D).
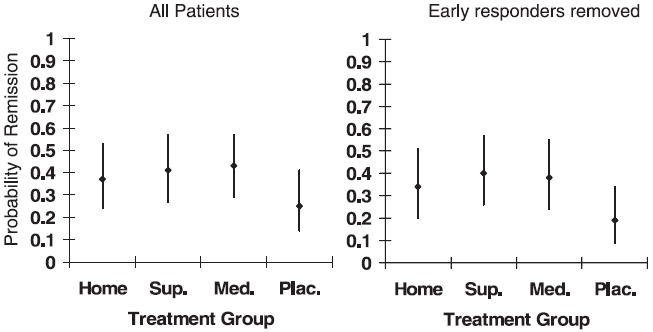
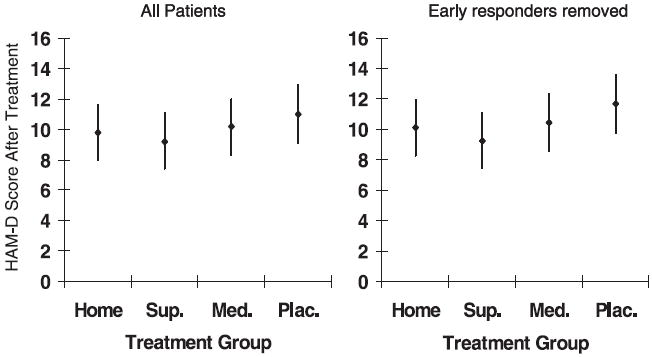
Results: After 4 months of treatment, 41% of the participants achieved remission, defined as no longer meeting the criteria for major depressive disorder (MDD) and a HAM-D score of <8. Patients receiving active treatments tended to have higher remission rates than the placebo controls: supervised exercise = 45%; home-based exercise = 40%; medication = 47%; placebo = 31% (p = .057). All treatment groups had lower HAM-D scores after treatment; scores for the active treatment groups were not significantly different from the placebo group (p = .23).
Conclusions: The efficacy of exercise in patients seems generally comparable with patients receiving antidepressant medication and both tend to be better than the placebo in patients with MDD. Placebo response rates were high, suggesting that a considerable portion of the therapeutic response is determined by patient expectations, ongoing symptom monitoring, attention, and other nonspecific factors.
Trial registration: ClinicalTrials.gov NCT00331305.
Figures
Comment in
-
Exercise, pharmacotherapy, and depression.Psychosom Med. 2008 Feb;70(2):263; author reply 264-5. doi: 10.1097/PSY.0b013e3181671bae. Epub 2008 Feb 6. Psychosom Med. 2008. PMID: 18256334 No abstract available.
-
Exercise in the treatment of major depressive disorder: still a long way to go.Psychosom Med. 2008 Feb;70(2):263; author reply 264-5. doi: 10.1097/PSY.0b013e31816726fa. Psychosom Med. 2008. PMID: 18276792 No abstract available.
References
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the national comorbidity survey replication. Arch Gen Psychiatry. 2005;62:593–602. - PubMed
-
- Agency for Health Care Policy and Research. Detection and diagnosis. Vol. 1. Rockville, MD: Department of Health and Human Services; 1993. Depression in primary care. UHCPR publication number 93-0550.
-
- Murray CJ, Lopez AD. Global mortality, disability, and the contribution of risk factors: global burden of disease study. Lancet. 1997;349:1436–42. - PubMed
-
- Insel TR, Charney DS. Research on major depression. JAMA. 2003;289:3167–8. - PubMed
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020. Global burden of disease study. Lancet. 1997;349:1498–504. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
