

The use of physical biomodelling in complex spinal surgery
- PMID: 17846803
- PMCID: PMC2200746
- DOI: 10.1007/s00586-006-0289-3
The use of physical biomodelling in complex spinal surgery
Abstract
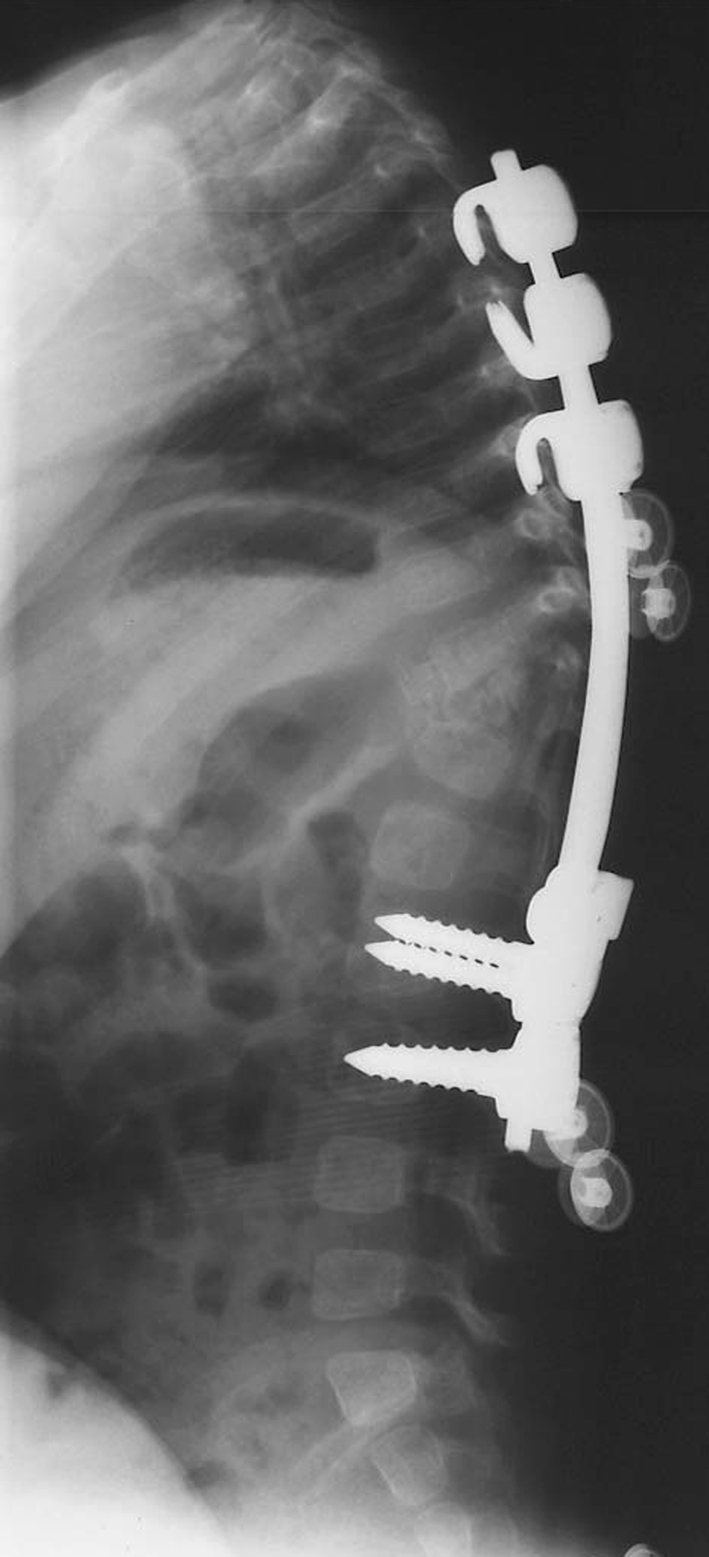
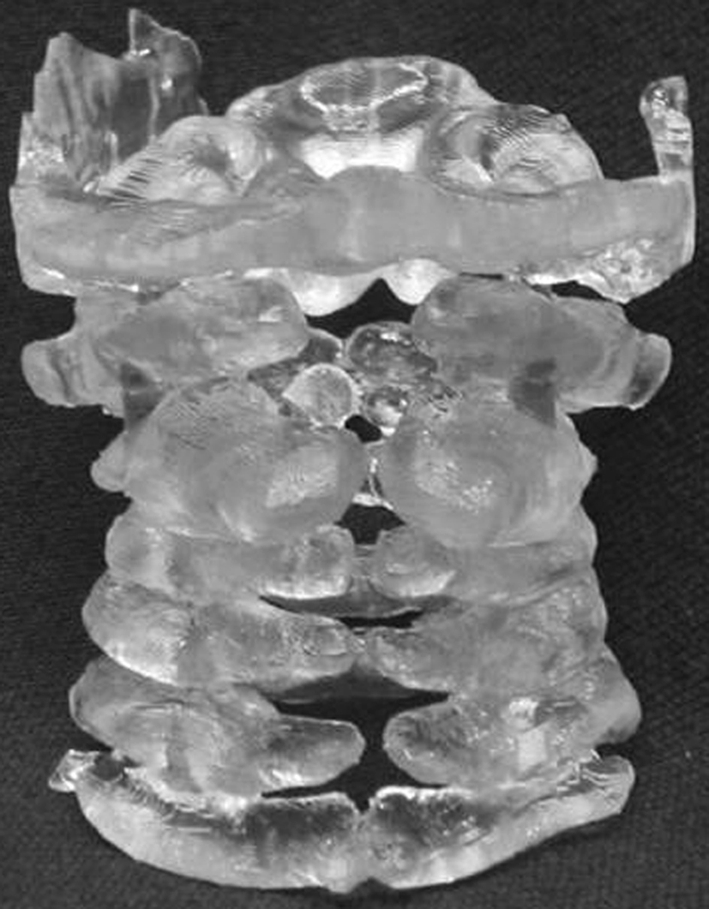
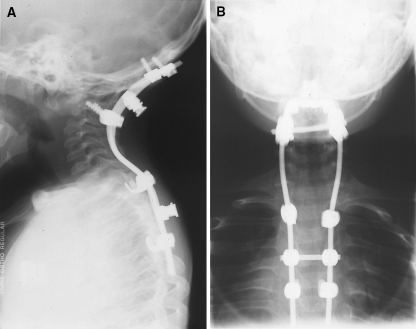
Prior studies have suggested that biomodels enhance patient education, preoperative planning and intra-operative stereotaxy; however, the usefulness of biomodels compared to regular imaging modalities such as X-ray, CT and MR has not been quantified. Our objective was to quantify the surgeon's perceptions on the usefulness of biomodels compared to standard visualisation modalities for preoperative planning and intra-operative anatomical reference. Physical biomodels were manufactured for a series of 26 consecutive patients with complex spinal pathologies using a stereolithographic technique based on CT data. The biomodels were used preoperatively for surgical planning and customising implants, and intra-operatively for anatomical reference. Following surgery, a detailed biomodel utility survey was completed by the surgeons, and informal telephone interviews were conducted with patients. Using biomodels, 21 deformity and 5 tumour cases were performed. Surgeons stated that the anatomical details were better visible on the biomodel than on other imaging modalities in 65% of cases, and exclusively visible on the biomodel in 11% of cases. Preoperative use of the biomodel led to a different decision regarding the choice of osteosynthetic materials used in 52% of cases, and the implantation site of osteosynthetic material in 74% of cases. Surgeons reported that the use of biomodels reduced operating time by a mean of 8% in tumour patients and 22% in deformity procedures. This study supports biomodelling as a useful, and sometimes essential tool in the armamentarium of imaging techniques used for complex spinal surgery.
Figures





References
-
- Barker TM, Earwaker WJS, Frost N, Wakeley G. Integration of 3-D medical imaging and rapid prototyping to create stereolithographic models. Aust Phys Eng Sci Med. 1993;16(2):79–85. - PubMed
-
- Bonnier L, Ayadi K, Vasdev A, Crouzet G, Raphael B. Three-dimensional reconstruction in routine computerized tomography of the skull and spine. J Neuroradiol. 1991;18(3):250–66. - PubMed
-
- D’Urso PS (1993) Stereolithographic modelling process [Australian Patent 684546; US Patent 5741215]
-
- D’Urso PS, Barker TM, Earwaker WJS, Bruce LJ, Atkinson L, Lanigan MW, Arvier JF, Effeney DJ. Stereolithographic biomodeling in cranio-maxillofacial surgery: a prospective trial. J Craniomaxillofac Surg. 1999;27(1):30–37. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
