

Benefit from preoperative radiotherapy in rectal cancer treatment: disease-free patients' and oncologists' preferences
- PMID: 17848910
- PMCID: PMC2360393
- DOI: 10.1038/sj.bjc.6603954
Benefit from preoperative radiotherapy in rectal cancer treatment: disease-free patients' and oncologists' preferences
Abstract
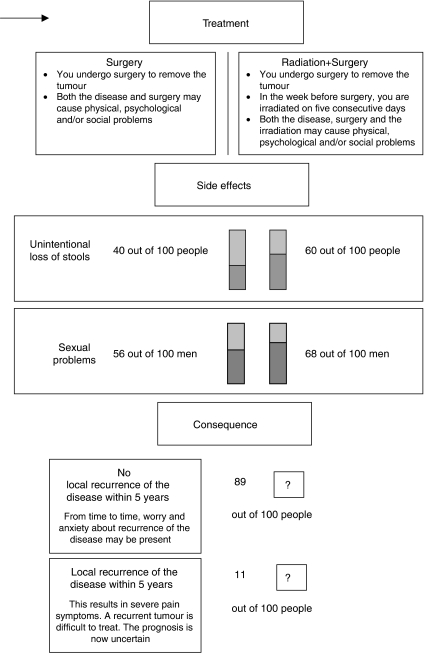
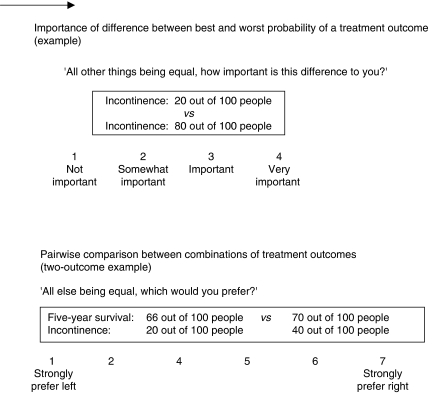
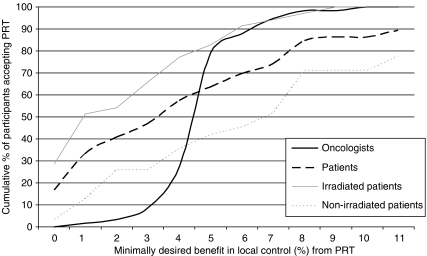
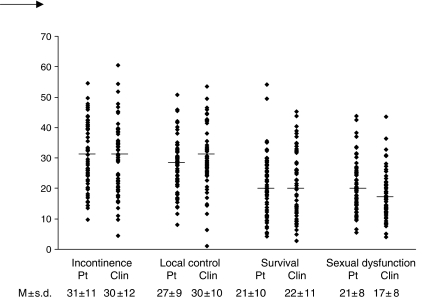
Preoperative radiotherapy (PRT) in resectable rectal cancer improves local control but increases probability of faecal incontinence and sexual dysfunction. Consensus was reached in 2001 in the Netherlands on a guideline advising PRT to new patients. Purpose was to assess at what benefit oncologists and rectal cancer patients prefer PRT followed by surgery to surgery alone, and how oncologists and patients value various treatment outcomes. Sixty-six disease-free patients and 60 oncologists (surgical, radiation, medical) were interviewed. Minimally desired benefit from PRT (local control) was assessed using the Treatment Tradeoff Method. Importance of survival, local control, faecal incontinence, and sexual dysfunction in determining treatment outcome preferences was assessed using Adaptive Conjoint Analysis. The range of required benefit from PRT varied widely within participant groups. Seventeen percent of patients would choose PRT at a 0% benefit; 11% would not choose PRT for the maximum benefit of 11%. Mean minimally desired benefit excluding these two groups was 4%. For oncologists, the required benefit was 5%. Also, how strongly participants valued treatment outcomes varied widely within groups. Of the four outcomes, participants considered incontinence most often as most important. Relative treatment outcome importance differed between specialties. Patients considered sexual functioning more important than oncologists. Large differences in treatment preferences exist between individual patients and oncologists. Oncologists should adequately inform their patients about the risks and benefits of PRT, and elicit patient preferences regarding treatment outcomes.
Figures
References
-
- ACA 5.0 Technical Paper (2005) www.sawtoothsoftware.com (Sawtooth Software Technical Paper Series)
-
- Beusterien KM, Dziekan K, Flood E, Harding G, Jordan JC (2005) Understanding patient preferences for HIV medications using adaptive conjoint analysis: feasibility assessment. Value Health 8: 453–461 - PubMed
-
- Birgisson H, Pahlman L, Gunnarsson U, Glimelius B (2005a) Adverse effects of preoperative radiation therapy for rectal cancer: long-term follow-up of the Swedish Rectal Cancer Trial. J Clin Oncol 23: 8697–8705 - PubMed
-
- Birgisson H, Pahlman L, Gunnarsson U, Glimelius B (2005b) Occurrence of second cancers in patients treated with radiotherapy for rectal cancer. J Clin Oncol 23: 6126–6131 - PubMed
-
- Bontenbal M, Nortier JW, Beex LV, Bakker P, Hupperets PS, Nooij MA, van Veelen H, Vreugdenhil G, Richel DJ, Blijham GH (2000) Adjuvant systemic therapy for patients with resectable breast cancer: guideline from the Dutch National Breast Cancer Platform and the Dutch Society for Medical Oncology. Ned Tijdschr Geneeskd 144: 984–989 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
