

Corticosteroids and increased risk of readmission after acute chest syndrome in children with sickle cell disease
- PMID: 17849474
- PMCID: PMC2757656
- DOI: 10.1002/pbc.21336
Corticosteroids and increased risk of readmission after acute chest syndrome in children with sickle cell disease
Abstract
Background: Acute chest syndrome (ACS) is a frequent cause of hospitalization and mortality in children with sickle cell disease. Transfusion is often required to prevent respiratory failure and treatment with dexamethasone may reduce the length of admission and the need for transfusions. We performed a retrospective cohort study to evaluate risk factors for readmission and prolonged hospitalization after different treatments for ACS.
Procedure: We identified patients <22 years of age hospitalized with ACS at Johns Hopkins Hospital from January 1998 to April 2004 using the hospitals discharge database and by reviewing dictated summaries.
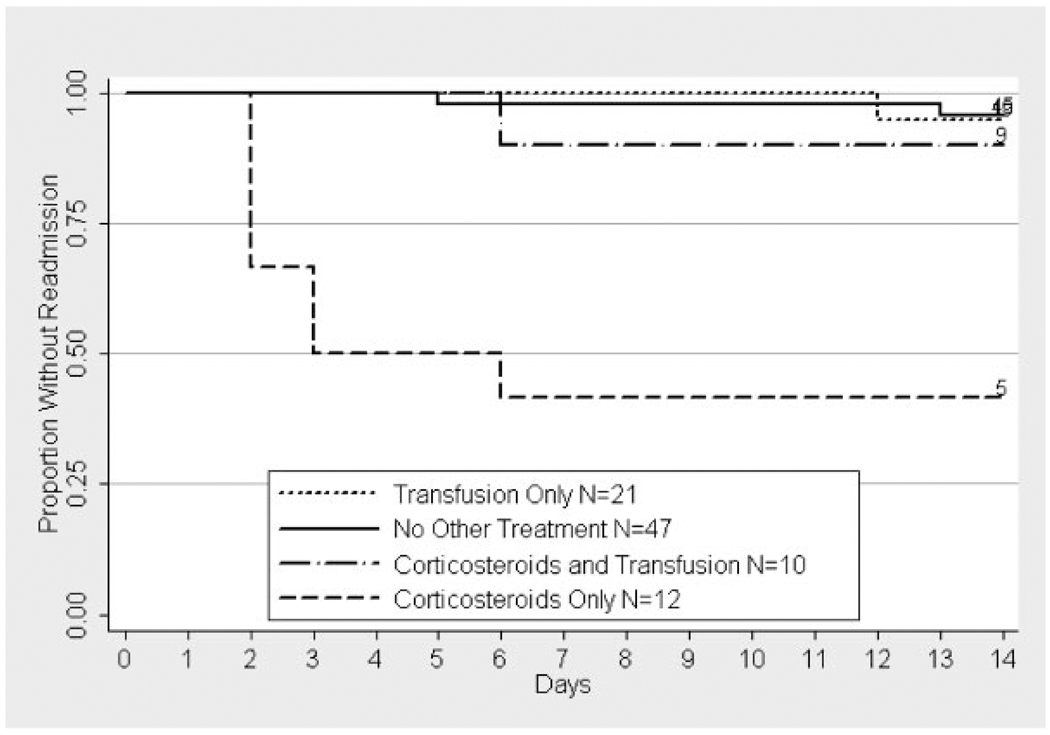
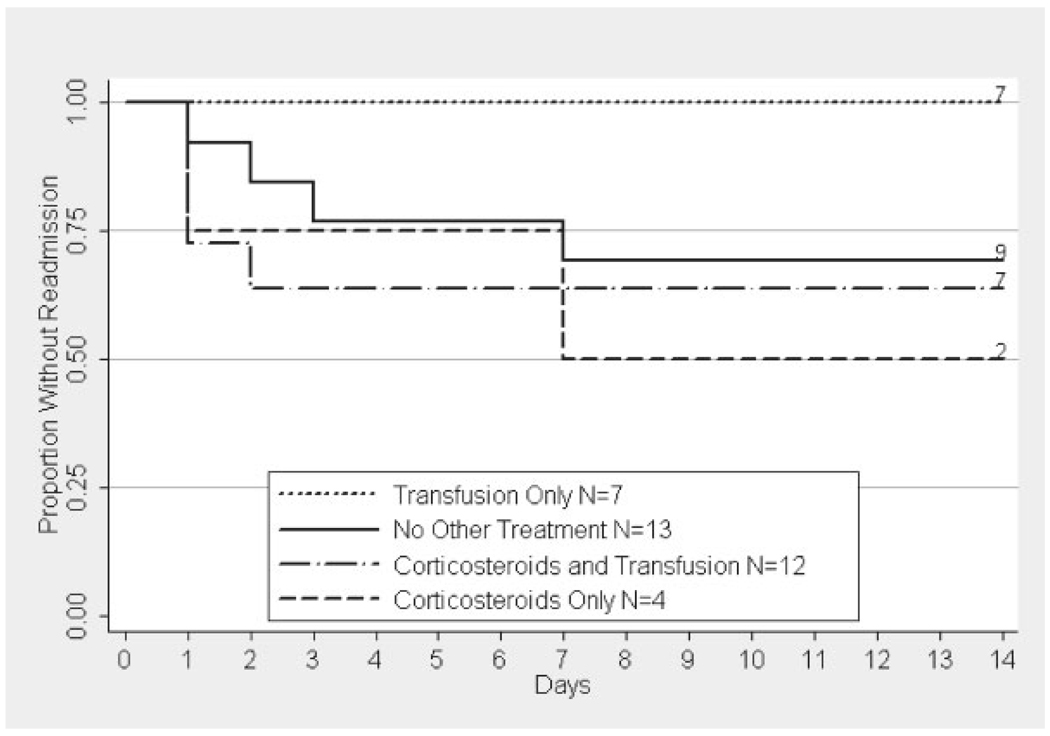
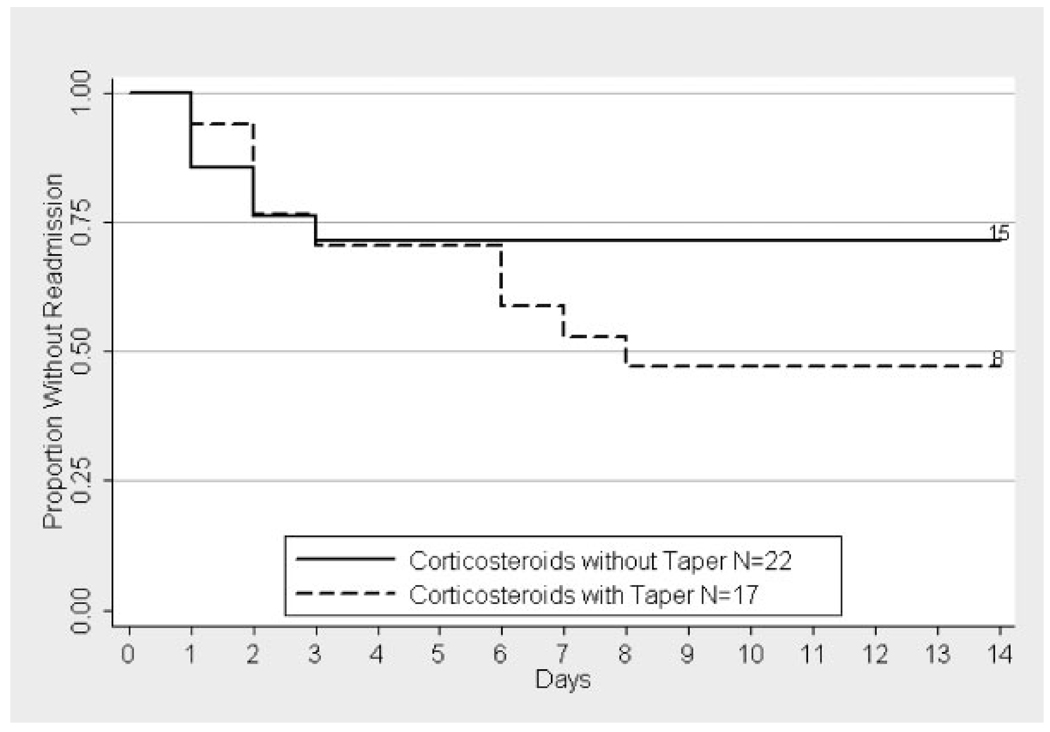
Results: We identified 65 patients with 129 episodes of ACS (mean age 12.5 years, range 1.2-21.9 years). Thirty-nine episodes were treated with corticosteroids and 51 with transfusions. Patients were readmitted within 14 days after 23 episodes (18%). Readmission was strongly associated with report of an inhaler or nebulizer at home [odds ratio (OR) 6.0, P < 0.05], diastolic BP at 48 hr (OR 1.8 per 10 mm increase, P<0.01), corticosteroids (OR 20, P < 0.005), or transfusion (OR 0.03, P < 0.05). Treatment with corticosteroids alone (P < 0.05) and older age (P < 0.001) were associated with longer hospitalization.
Conclusions: These results demonstrate a greatly elevated independent risk of readmission after ACS in children with asthma and after treatment with corticosteroids and a protective effect of transfusion. Although dexamethasone has documented efficacy for reducing the duration of ACS, the substantial risk of readmission for pain should limit its use.
(c) 2008 Wiley-Liss, Inc.
Figures
References
-
- Bernini JC, Rogers ZR, Sandler ES, et al. Beneficial effect of intravenous dexamethasone in children with mild to moderately severe acute chest syndrome complicating sickle cell disease. Blood. 1998;92:3082–3089. - PubMed
-
- Vichinsky EP, Neumayr LD, Earles AN, et al. National Acute Chest Syndrome Study Group. Causes and outcomes of the acute chest syndrome in sickle cell disease. N Engl J Med. 2000;342:1855–1865. - PubMed
-
- Castro O, Brambilla DJ, Thorington B, et al. The Cooperative Study of Sickle Cell Disease. The acute chest syndrome in sickle cell disease: Incidence and risk factors. Blood. 1994;84:643–649. - PubMed
-
- Vichinsky EP, Styles LA, Colangelo LH, et al. Cooperative Study of Sickle Cell Disease. Acute chest syndrome in sickle cell disease: Clinical presentation and course. Blood. 1997;89:1787–1792. - PubMed
-
- Platt OS, Brambilla DJ, Rosse WF, et al. Mortality in sickle cell disease—Life expectancy and risk factors for early death. N Engl J Med. 1994;330:1639–1644. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
