

One-year health status outcomes of unstable angina versus myocardial infarction: a prospective, observational cohort study of ACS survivors
- PMID: 17850662
- PMCID: PMC2014769
- DOI: 10.1186/1471-2261-7-28
One-year health status outcomes of unstable angina versus myocardial infarction: a prospective, observational cohort study of ACS survivors
Abstract
Background: Unstable angina (UA) patients have lower mortality and reinfarction risks than ST-elevation (STEMI) or non-ST elevation myocardial infarction (NSTEMI) patients and, accordingly, receive less aggressive treatment. Little is known, however, about the health status outcomes (angina, physical function, and quality of life) of UA versus MI patients among survivors of an ACS hospitalization.
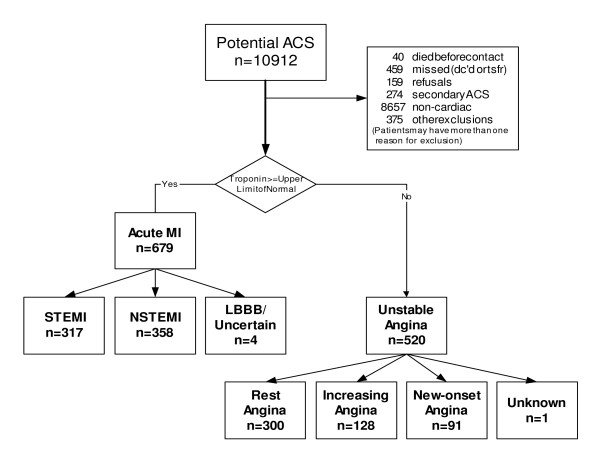
Methods: In a cohort of 1,192 consecutively enrolled ACS survivors from two Kansas City hospitals, we evaluated the associations between ACS presentation (UA, NSTEMI, and STEMI) and one-year health status (angina, physical functioning and quality of life), one-year cardiac rehospitalization rates, and two-year mortality outcomes, using multivariable regression modeling.
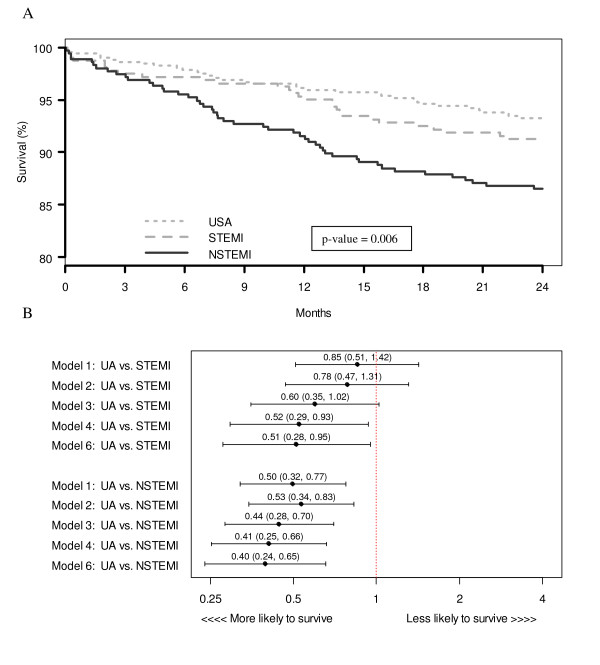
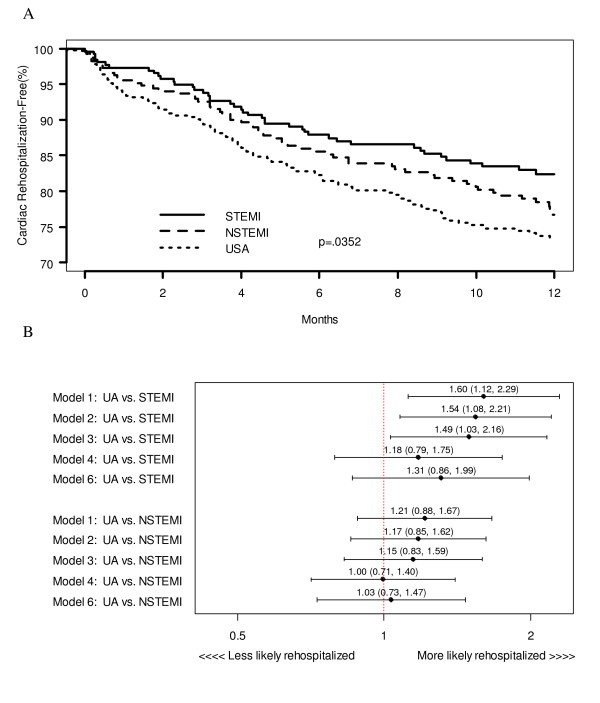
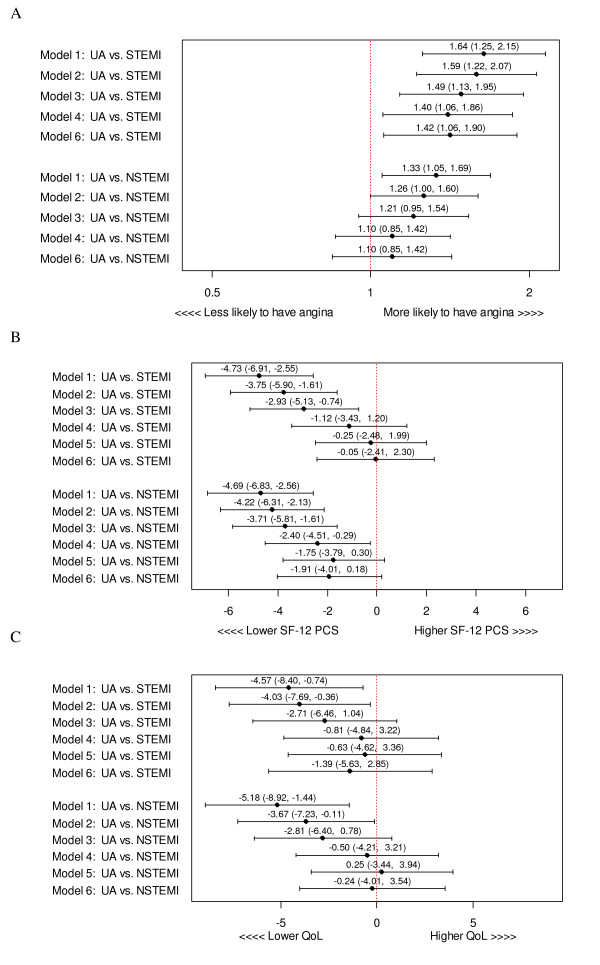
Results: After multivariable adjustment for demographic, hospital, co-morbidity, baseline health status, and treatment characteristics, UA patients had a greater prevalence of angina at 1 year than STEMI patients (adjusted relative risk [RR] = 1.42; 95% CI [1.06, 1.90]) and similar rates as NSTEMI patients (adjusted RR = 1.1; 95% CI [0.85, 1.42]). In addition, UA patients fared no better than MI patients in Short Form-12 physical component scores (UA vs. STEMI score difference -0.05 points; 95% CI [-2.41, 2.3]; UA vs. NSTEMI score difference -1.91 points; 95% CI [-4.01, 0.18]) or Seattle Angina Questionnaire quality of life scores (UA vs. STEMI score difference -1.39 points; 95% CI [-5.63, 2.85]; UA vs. NSTEMI score difference -0.24 points 95% CI [-4.01, 3.54]). Finally, UA patients had similar rehospitalization rates as MI patients (UA vs. STEMI adjusted hazard ratio [HR] = 1.31; 95% CI [0.86, 1.99]; UA vs. NSTEMI adjusted HR = 1.03; 95% CI [0.73, 1.47]), despite better 2-year survival (UA vs. STEMI adjusted HR = 0.51; 95% confidence interval (CI) [0.28, 0.95]; UA vs. NSTEMI adjusted HR = 0.40; 95% CI [0.24, 0.65]).
Conclusion: Although UA patients have better survival rates, they have similar or worse one-year health status outcomes and cardiac rehospitalization rates as compared with MI patients. Clinicians should be aware of the adverse health status outcome risks for UA patients and consider close monitoring for the opportunity to improve their health status and minimize the need for subsequent rehospitalization.
Figures
References
-
- Armstrong PW, Fu Y, Chang WC, Topol EJ, Granger CB, Betriu A, Van de Werf F, Lee KL, Califf RM. Acute coronary syndromes in the GUSTO-IIb trial: prognostic insights and impact of recurrent ischemia. The GUSTO-IIb Investigators. Circulation. 1998;98:1860–8. - PubMed
-
- Furman MI, Dauerman HL, Goldberg RJ, Yarzebski J, Lessard D, Gore JM. Twenty-two year (1975 to 1997) trends in the incidence, in-hospital and long-term case fatality rates from initial Q-wave and non-Q-wave myocardial infarction: a multi-hospital, community-wide perspective. J Am Coll Cardiol. 2001;37:1571–80. doi: 10.1016/S0735-1097(01)01203-7. - DOI - PubMed
-
- Rogers WJ, Canto JG, Lambrew CT, Tiefenbrunn AJ, Kinkaid B, Shoultz DA, Frederick PD, Every N. Temporal trends in the treatment of over 1.5 million patients with myocardial infarction in the US from 1990 through 1999: the National Registry of Myocardial Infarction 1, 2 and 3. J Am Coll Cardiol. 2000;36:2056–63. doi: 10.1016/S0735-1097(00)00996-7. - DOI - PubMed
-
- Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, Van de Werf F, Goodman SG, Granger CB, Steg PG, Gore JM, Budaj A, Avezum A, Flather MD, Fox KA. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. Jama. 2004;291:2727–33. doi: 10.1001/jama.291.22.2727. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
