

Dual-source computed tomography in patients with acute chest pain: feasibility and image quality
- PMID: 17851666
- PMCID: PMC2077913
- DOI: 10.1007/s00330-007-0724-9
Dual-source computed tomography in patients with acute chest pain: feasibility and image quality
Abstract
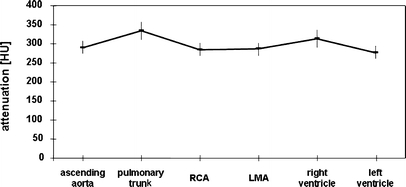
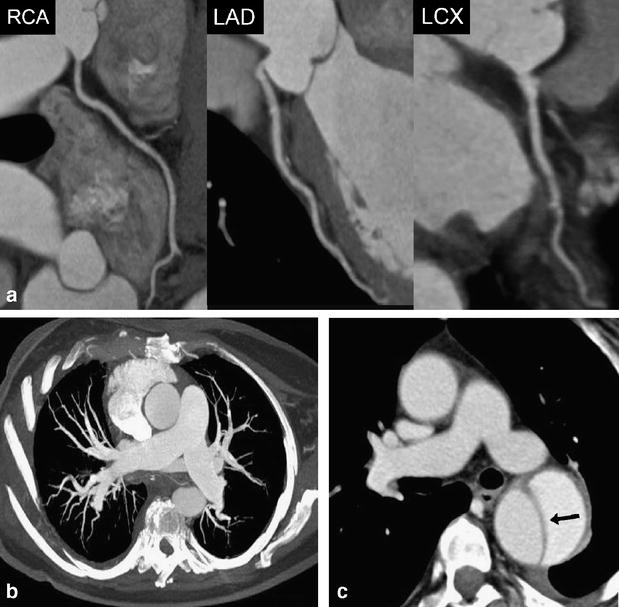
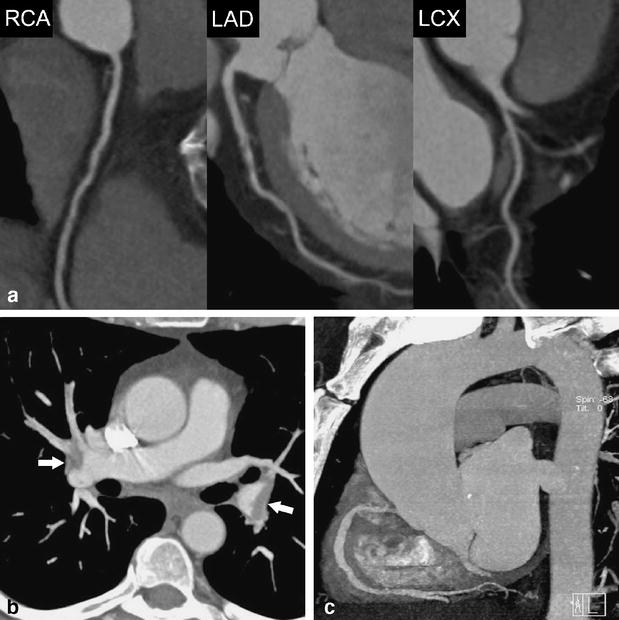
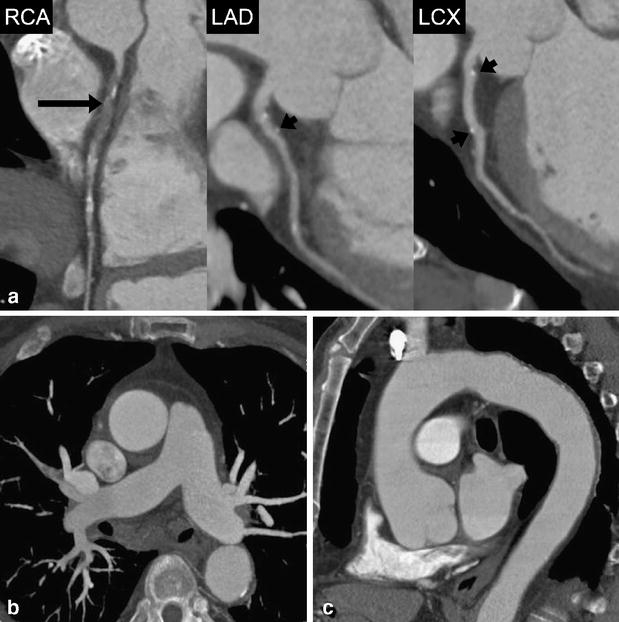
The aim of this study was to determine the feasibility and image quality of dual-source computed tomography angiography (DSCTA) in patients with acute chest pain for the assessment of the lung, thoracic aorta, and for pulmonary and coronary arteries. Sixty consecutive patients (32 female, 28 male, mean age 58.1+/-16.3 years) with acute chest pain underwent contrast-enhanced electrocardiography-gated DSCTA without prior beta-blocker administration. Vessel attenuation of different thoracic vascular territories was measured, and image quality was semi-quantitatively analyzed by two independent readers. Image quality of the thoracic aorta was diagnostic in all 60 patients, image quality of pulmonary arteries was diagnostic in 59, and image quality of coronary arteries was diagnostic in 58 patients. Pairwise intraindividual comparisons of attenuation values were small and ranged between 1+/-6 HU comparing right and left coronary artery and 56+/-9 HU comparing the pulmonary trunk and left ventricle. Mean attenuation was 291+/-65 HU in the ascending aorta, 334+/-93 HU in the pulmonary trunk, and 285+/-66 HU and 268+/-67 HU in the right and left coronary artery, respectively. DSCTA is feasible and provides diagnostic image quality of the thoracic aorta, pulmonary and coronary arteries in patients with acute chest pain.
Figures
References
-
- Zimmerman J et al (1999) Diagnostic marker cooperative study for the diagnosis of myocardial infarction. Circulation 99:1671–1677 - PubMed
