

Maternal serum soluble CD30 is increased in normal pregnancy, but decreased in preeclampsia and small for gestational age pregnancies
- PMID: 17853188
- PMCID: PMC2276339
- DOI: 10.1080/14767050701482993
Maternal serum soluble CD30 is increased in normal pregnancy, but decreased in preeclampsia and small for gestational age pregnancies
Abstract
Objective: Women with preeclampsia and those who deliver small for gestational age (SGA) neonates are characterized by intravascular inflammation (T helper 1 (Th1)-biased immune response). There is controversy about the T helper 2 (Th2) response in preeclampsia and SGA. CD30, a member of the tumor necrosis factor receptor superfamily, is preferentially expressed in vitro and in vivo by activated T cells producing Th2-type cytokines. Its soluble form (sCD30) has been proposed to be an index of Th2 immune response. The objective of this study was to determine whether the maternal serum concentration of sCD30 changes with normal pregnancy, as well as in mothers with preeclampsia and those who deliver SGA neonates.
Methods: This cross-sectional study included patients in the following groups: (1) non-pregnant women (N = 49); (2) patients with a normal pregnancy (N = 89); (3) patients with preeclampsia (N = 100); and (4) patients who delivered an SGA neonate (N = 78). Maternal serum concentration of sCD30 was measured by a specific and sensitive enzyme-linked immunoassay. Non-parametric tests with post-hoc analysis were used for comparisons. A p value <0.05 was considered statistically significant.
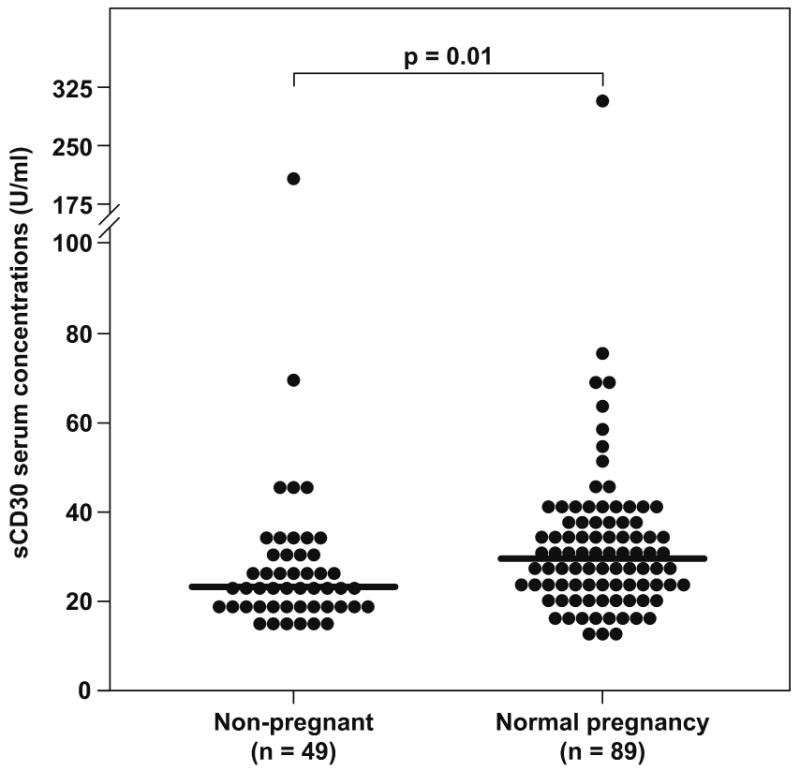
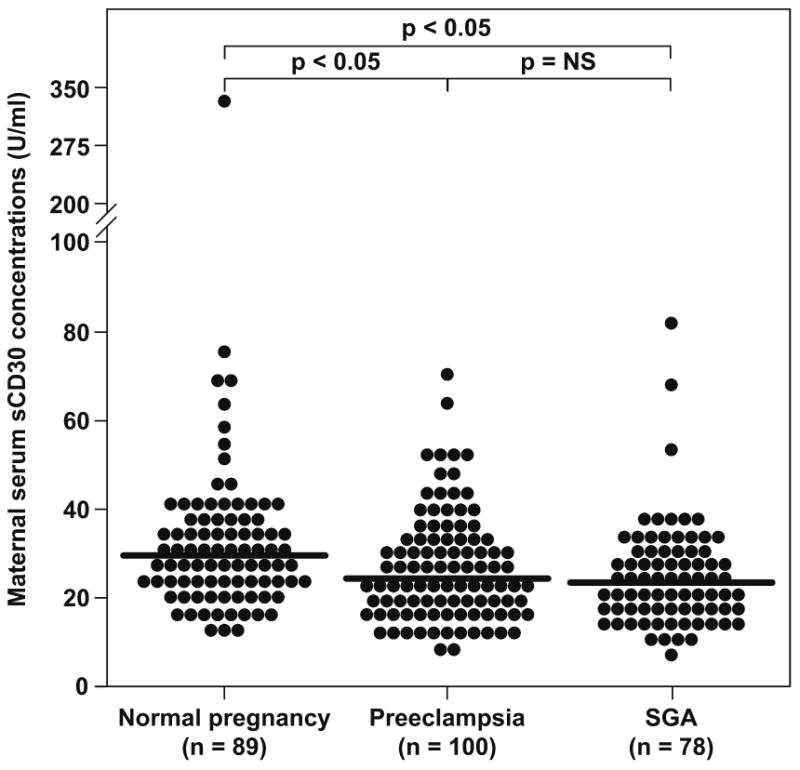
Results: (1) The median sCD30 serum concentration of pregnant women was significantly higher than that of non-pregnant women (median 29.7 U/mL, range 12.2-313.2 vs. median 23.2 U/mL, range 14.6-195.1, respectively; p = 0.01). (2) Patients with preeclampsia had a significantly lower median serum concentration of sCD30 than normal pregnant women (median 24.7 U/mL, range 7.6-71.2 vs. median 29.7 U/mL, range 12.2-313.2, respectively; p < 0.05). (3) Mothers with SGA neonates had a lower median concentration of sCD30 than normal pregnant women (median 23.4 U/mL, range 7.1-105.3 vs. median 29.7 U/mL, range 12.2-313.2, respectively; p < 0.05). (4) There was no significant correlation (r = -0.059, p = 0.5) between maternal serum sCD30 concentration and gestational age (19-38 weeks) in normal pregnant women.
Conclusions: (1) Patients with preeclampsia and those who deliver an SGA neonate had a significantly lower serum concentration of sCD30 than normal pregnant women. (2) This finding is consistent with the view that preeclampsia and SGA are associated with a polarized Th1 immune response and, perhaps, a reduced Th2 response.
Figures
Similar articles
-
Maternal serum soluble CD30 is increased in pregnancies complicated with acute pyelonephritis.J Matern Fetal Neonatal Med. 2007 Nov;20(11):803-11. doi: 10.1080/14767050701492851. J Matern Fetal Neonatal Med. 2007. PMID: 17853184 Free PMC article.
-
Preeclampsia and small-for-gestational age are associated with decreased concentrations of a factor involved in angiogenesis: soluble Tie-2.J Matern Fetal Neonatal Med. 2008 Jun;21(6):389-402. doi: 10.1080/14767050802046069. J Matern Fetal Neonatal Med. 2008. PMID: 18570117 Free PMC article.
-
CXCL10/IP-10: a missing link between inflammation and anti-angiogenesis in preeclampsia?J Matern Fetal Neonatal Med. 2007 Nov;20(11):777-92. doi: 10.1080/14767050701483298. J Matern Fetal Neonatal Med. 2007. PMID: 17943641 Free PMC article.
-
Leukocytes of pregnant women with small-for-gestational age neonates have a different phenotypic and metabolic activity from those of women with preeclampsia.J Matern Fetal Neonatal Med. 2010 Jun;23(6):476-87. doi: 10.3109/14767050903216033. J Matern Fetal Neonatal Med. 2010. PMID: 19916874 Free PMC article.
-
Inflammation and pregnancy: the role of the immune system at the implantation site.Ann N Y Acad Sci. 2011 Mar;1221(1):80-7. doi: 10.1111/j.1749-6632.2010.05938.x. Ann N Y Acad Sci. 2011. PMID: 21401634 Free PMC article. Review.
Cited by
-
Maternal plasma concentrations of angiogenic/anti-angiogenic factors are of prognostic value in patients presenting to the obstetrical triage area with the suspicion of preeclampsia.J Matern Fetal Neonatal Med. 2011 Oct;24(10):1187-207. doi: 10.3109/14767058.2011.589932. Epub 2011 Aug 9. J Matern Fetal Neonatal Med. 2011. PMID: 21827221 Free PMC article.
-
Microbial invasion of the amniotic cavity in pregnancies with small-for-gestational-age fetuses.J Perinat Med. 2010 Sep;38(5):495-502. doi: 10.1515/jpm.2010.076. J Perinat Med. 2010. PMID: 20482466 Free PMC article.
-
Maternal plasma soluble TRAIL is decreased in preeclampsia.J Matern Fetal Neonatal Med. 2014 Feb;27(3):217-27. doi: 10.3109/14767058.2013.806906. Epub 2013 Aug 13. J Matern Fetal Neonatal Med. 2014. PMID: 23688319 Free PMC article.
-
Placental lesions associated with maternal underperfusion are more frequent in early-onset than in late-onset preeclampsia.J Perinat Med. 2011 Nov;39(6):641-52. doi: 10.1515/jpm.2011.098. Epub 2011 Aug 17. J Perinat Med. 2011. PMID: 21848483 Free PMC article.
-
Proteomic analysis of serum in lung cancer induced by 3-methylcholanthrene.J Biomed Biotechnol. 2009;2009:397910. doi: 10.1155/2009/397910. Epub 2009 Sep 24. J Biomed Biotechnol. 2009. PMID: 19794824 Free PMC article.
References
-
- Romero R. Prenatal medicine: The child is the father of the man. Prenatal and Neonatal Medicine. 1996;1:8–11. - PubMed
-
- Sibai BM, Gordon T, Thom E, Caritis SN, Klebanoff M, McNellis D, Paul RH. Risk factors for preeclampsia in healthy nulliparous women: A prospective multicenter study. American Journal Of Obstetrics And Gynecology. 1995;172:642–648. - PubMed
-
- Jacobsson B, Ladfors L, Milsom I. Advanced maternal age and adverse perinatal outcome. Obstet Gynecol. 2004;104:727–733. - PubMed
-
- Odibo AO, Nelson D, Stamilio DM, Sehdev HM, Macones GA. Advanced maternal age is an independent risk factor for intrauterine growth restriction. Am J Perinatol. 2006;23:325–328. - PubMed
-
- Rey E, Couturier A. The prognosis of pregnancy in women with chronic hypertension. American Journal Of Obstetrics And Gynecology. 1994;171:410–416. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources