

Transformation of cytogenetically normal chronic myelomonocytic leukaemia to an acute myeloid leukaemia and the emergence of a novel +13, +15 double trisomy resulting in an adverse outcome
- PMID: 17853637
- PMCID: PMC2075573
Transformation of cytogenetically normal chronic myelomonocytic leukaemia to an acute myeloid leukaemia and the emergence of a novel +13, +15 double trisomy resulting in an adverse outcome
Abstract
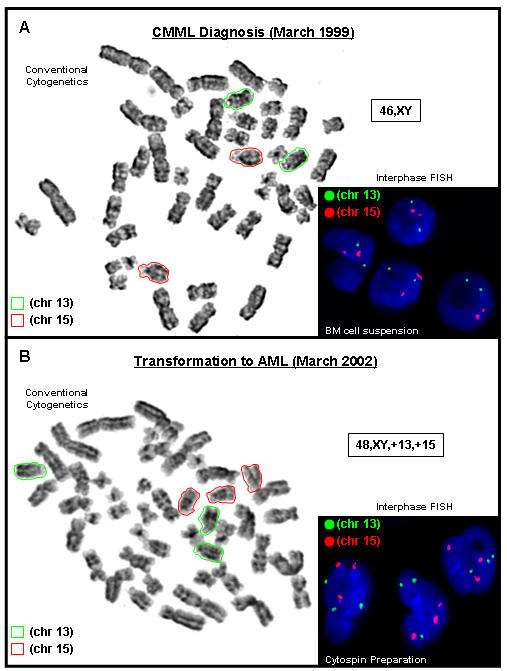
A 58-year-old man was admitted with symptoms of lethargy and easy bruising for four months duration. Peripheral blood (PB) analysis revealed a white blood cell count (WBC) of 15.9 x 10(9)/l with monocytes 5.4 x 10(9)/l. Bone marrow (BM) was hypercellular with 15% blasts, monocytosis and trilineage dysplasia. Conventional cytogenetic analysis (G-banding) detected an apparently normal male karyotype (46,XY). A diagnosis of chronic myelomonocytic leukaemia (CMML) was made. After 3 years, PB analysis revealed a WBC count of 22 x 10(9)/l and a predominance of blasts. BM aspirate analysis also revealed 89% myeloid blasts and G-banding detected the emergence of an abnormal clone harbouring an extra copy of chromosomes 13 and 15. A diagnosis of disease transformation to acute myeloid leukaemia (AML) was made. Post chemotherapy BM aspirate was very hypocellular and the abnormal +13, +15 clone was still present suggesting primary refractory disease. A second course of chemotherapy was only administered for 24 hours due to complications. The abnormal +13, +15 clone was still present and it was decided that no further treatment apart from palliative care could be offered. The patient died 11 weeks later, five months after AML transformation. This is the first description of a cytogenetically normal CMML patient transforming to AML with the emergence of a unique +13, +15 double trisomy resulting in an adverse outcome.
Figures
Similar articles
-
Trisomy 14 in myelodysplastic syndromes: report of two cases and review of the literature.Arch Pathol Lab Med. 1998 Jan;122(1):77-83. Arch Pathol Lab Med. 1998. PMID: 9448022 Review.
-
The role of peripheral blood, bone marrow aspirate and especially bone marrow trephine biopsy in distinguishing atypical chronic myeloid leukemia from chronic granulocytic leukemia and chronic myelomonocytic leukemia.Eur J Haematol. 2009 Oct;83(4):292-301. doi: 10.1111/j.1600-0609.2009.01283.x. Epub 2009 Jun 2. Eur J Haematol. 2009. PMID: 19500135
-
[Fluorescence in situ hybridization studies on a myeloid leukemia patient with ins(8;21)(q22;q22.1q22.3)].Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2009 Apr;26(2):203-6. doi: 10.3760/cma.j.issn.1003-9406.2009.02.019. Zhonghua Yi Xue Yi Chuan Xue Za Zhi. 2009. PMID: 19350517 Chinese.
-
Trisomy 13 and myeloid malignancy--characteristic blast cell morphology: a United Kingdom Cancer Cytogenetics Group survey.Br J Haematol. 1998 Jun;101(4):749-52. doi: 10.1046/j.1365-2141.1998.00760.x. Br J Haematol. 1998. PMID: 9674750
-
Trisomy 19 as the sole chromosomal anomaly in hematologic neoplasms.Cancer Genet Cytogenet. 1994 May;74(1):62-5. doi: 10.1016/0165-4608(94)90031-0. Cancer Genet Cytogenet. 1994. PMID: 8194050 Review.
Cited by
-
Targeted Therapy Development in Acute Myeloid Leukemia.Biomedicines. 2023 Feb 20;11(2):641. doi: 10.3390/biomedicines11020641. Biomedicines. 2023. PMID: 36831175 Free PMC article. Review.
-
Role of Gene Mutations in Acute Myeloid Leukemia: A Review Article.Glob Med Genet. 2023 Jun 23;10(2):123-128. doi: 10.1055/s-0043-1770768. eCollection 2023 Jun. Glob Med Genet. 2023. PMID: 37360004 Free PMC article. Review.
-
LC-MS/MS method for the quantitation of decitabine and venetoclax in rat plasma after SPE: Application to pharmacokinetic study.Saudi Pharm J. 2023 Sep;31(9):101693. doi: 10.1016/j.jsps.2023.06.026. Epub 2023 Jul 4. Saudi Pharm J. 2023. PMID: 37559870 Free PMC article.
References
-
- Aul C, Gattermann N, Schneider W. Epidemiological and etiological aspects of myelodysplastic syndromes. Leuk Lymphoma. 1995;16(3–4):247–62. - PubMed
-
- Aul C, Bowen DT, Yoshida Y. Pathogenesis, etiology and epidemiology of myelodysplastic syndromes. Haematologica. 1998;83(1):71–86. - PubMed
-
- Bennett JM, Catovsky D, Daniel MT, Flandrin G, Galton DA, Gralnick HR, et al. Proposals for the classification of the myelodysplastic syndromes. Br J Haematol. 1982;51(2):189–99. - PubMed
-
- Harris NL, Jaffe ES, Diebold J, Flandrin G, Muller-Hermelink HK, Vardiman J, et al. The World Health Organization classification of hematological malignancies: report of the Clinical Advisory Committee meeting - Airlie House, Virginia, November 1997. J Clin Oncol. 1999;17(12):3835–49. - PubMed
-
- Bennett JM. WHO-classification of the acute leukemias and myelodysplastic syndromes. Int J Hematol. 2000;72(2):131–3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources