

The role of surgical audit in improving patient management; nasal haemorrhage: an audit study
- PMID: 17854499
- PMCID: PMC2034528
- DOI: 10.1186/1471-2482-7-19
The role of surgical audit in improving patient management; nasal haemorrhage: an audit study
Abstract
Background: Nasal bleeding remains one of the most common Head & Neck Surgical (Ear Nose and Throat [ENT]/Oral & Maxillofacial Surgery [OMFS]) emergencies resulting in hospital admission. In the majority of cases, no other intervention is required other than nasal packing, and it was felt many cases could ideally be managed at home, without further medical interference. A limited but national telephone survey of accident and emergency departments revealed that early discharge practice was identified in some rural areas and urban departments (where adverse socio-demographic factors resulted in poor patient compliance to admission or follow up), with little adverse patient sequelae. A simple nasal packing protocol was also identified. The aim of this audit was to determine if routine nasal haemorrhage (epistaxis) can be managed at home with simple nasal packing; a retrospective and prospective audit. Ethical committee approval was obtained. Similar practice was identified in other UK accident and emergency centres. Literature was reviewed and best practice identified. Regional consultation and feedback with regard to prospective changes and local applicability of areas of improved practice mutually agreed upon with involved providers of care.
Methods: Retrospective: The Epistaxis admissions for the previous four years during the same seven months (September to March). Prospective: 60 consecutive patients referred with a diagnosis of Nasal bleeding over a seven month time course (September to March). All patients were over 16, not pregnant and gave fully informed counselled consent. New Guidelines for the management of nosebleeds, nasal packing protocols (with Netcel) and discharge policy were developed at the Hospital. Training of accident and emergency and emergency ENT staff was provided together with access to adequate examination and treatment resources. Detailed patient information leaflets were piloted and developed for use.
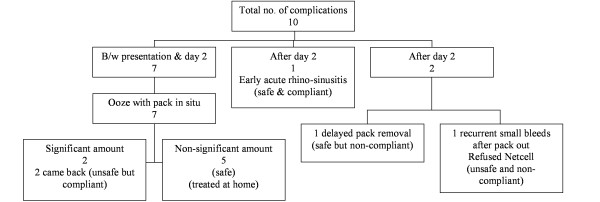
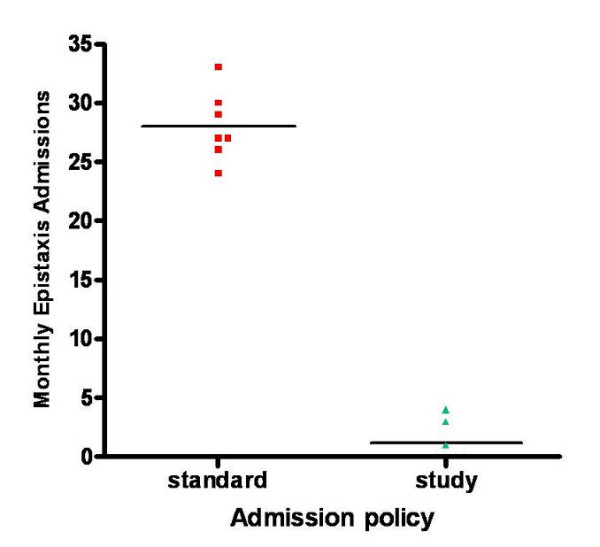
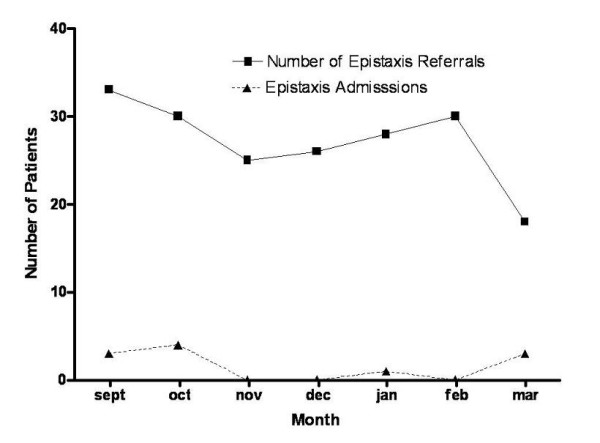
Results: Previously all patients requiring nasal packing were admitted. The type of nasal packing included Gauge impregnated Bismuth Iodoform Paraffin Paste, Nasal Tampon, and Vaseline gauge. Over the previous four year period (September to March) a mean of 28 patients were admitted per month, with a mean duration of in patient stay of 2.67 days. In the prospective audit the total number of admissions was significantly reduced, by over 70%, (chi2 = 25.05, df = 6, P < 0.0001), despite no significant change in the number of monthly epistaxis referrals (chi2 = 4.99, df = 6, P < 0.0001). There was also a significant increase in the mean age of admitted patients with epistaxis (chi2 = 22.71, df = 5, P < 0.0001), the admitted patients had a mean length of stay of 2.53 days. This policy results is an estimated saved 201.39 bed days per annum resulting in an estimated annual speciality saving of over pound 50,000, allowing resource re-allocation to other areas of need. Furthermore, bed usage could be optimised for other emergency or elective work.
Conclusion: Exclusion criteria have now been expanded to exclude traumatic nasal haemorrhage. New adjunctive therapies now include direct endoscopic bipolar diathermy of bleeding points, and the judicious use of topical pro-coagulant agents applied via the nasal tampon. Expansion of the audit protocols for use in general practice.This original audit informed clinical practice and had potential benefits for patients, clinicians, and provision of service. Systematic replication of this project, possibly on a regional and general practice basis, could result in further financial savings, which would allow development of improved patient services and delivery of care.
Figures
Similar articles
-
A change in UK epistaxis management.Eur Arch Otorhinolaryngol. 2008 Nov;265(11):1349-54. doi: 10.1007/s00405-008-0657-1. Epub 2008 Apr 8. Eur Arch Otorhinolaryngol. 2008. PMID: 18392840
-
Do all epistaxis patients with a nasal pack need admission? A retrospective study of 116 patients managed in accident and emergency according to a peer reviewed protocol.J Laryngol Otol. 2007 Mar;121(3):222-7. doi: 10.1017/S0022215106003148. Epub 2006 Oct 11. J Laryngol Otol. 2007. PMID: 17040607
-
Clinical Practice Guideline: Nosebleed (Epistaxis).Otolaryngol Head Neck Surg. 2020 Jan;162(1_suppl):S1-S38. doi: 10.1177/0194599819890327. Otolaryngol Head Neck Surg. 2020. PMID: 31910111
-
Clinical Practice Guideline: Nosebleed (Epistaxis) Executive Summary.Otolaryngol Head Neck Surg. 2020 Jan;162(1):8-25. doi: 10.1177/0194599819889955. Otolaryngol Head Neck Surg. 2020. PMID: 31910122 Review.
-
Recent trends in epistaxis management in the United States: 2008-2010.JAMA Otolaryngol Head Neck Surg. 2013 Dec;139(12):1279-84. doi: 10.1001/jamaoto.2013.5220. JAMA Otolaryngol Head Neck Surg. 2013. PMID: 24136624 Review.
Cited by
-
One Year Audit of In Patient Department of Oral and Maxillofacial Surgery, Dhaka Dental College Hospital.J Maxillofac Oral Surg. 2016 Jun;15(2):229-35. doi: 10.1007/s12663-015-0822-1. Epub 2015 Aug 19. J Maxillofac Oral Surg. 2016. PMID: 27298547 Free PMC article.
-
Epidemiological profile of otorhinolaryngological emergencies at a medical college, in rural area of gujarat.Indian J Otolaryngol Head Neck Surg. 2012 Sep;64(3):218-24. doi: 10.1007/s12070-011-0293-8. Epub 2011 Aug 28. Indian J Otolaryngol Head Neck Surg. 2012. PMID: 23998023 Free PMC article.
-
A change in UK epistaxis management.Eur Arch Otorhinolaryngol. 2008 Nov;265(11):1349-54. doi: 10.1007/s00405-008-0657-1. Epub 2008 Apr 8. Eur Arch Otorhinolaryngol. 2008. PMID: 18392840
-
How participation in surgical mortality audit impacts surgical practice.BMC Surg. 2017 Apr 19;17(1):42. doi: 10.1186/s12893-017-0240-z. BMC Surg. 2017. PMID: 28424055 Free PMC article.
-
A 5-year audit of major maxillofacial surgeries at Usmanu Danfodiyo university teaching hospital, Nigeria.BMC Health Serv Res. 2018 Jun 7;18(1):416. doi: 10.1186/s12913-018-3236-1. BMC Health Serv Res. 2018. PMID: 29879975 Free PMC article.
References
-
- Hippocrates (5th Century BC), Translated by Adams F St Petersburg Med Wchnschr. 1877. p. 302.
-
- Chaiyasate S, Roongrotwattanasiri K, Fooanan S, Sumitsawan Y. Epistaxis in Chiang Mai University Hospital. J Med Assoc Thai. 2005;88:1282–6. - PubMed
-
- Klossek JM, Dufour X, de Montreuil CB, Fontanel JP, Peynegre R, Reyt E, Rugina M, Samardzic M, Serrano E, Stoll D, Chevillard C. Epistaxis and its management: an observational pilot study carried out in 23 hospital centres in France. Rhinology. 2006;44:151–5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
