

Liver function after irradiation based on computed tomographic portal vein perfusion imaging
- PMID: 17855011
- PMCID: PMC2714771
- DOI: 10.1016/j.ijrobp.2007.05.078
Liver function after irradiation based on computed tomographic portal vein perfusion imaging
Abstract
Purpose: To determine whether individual and regional liver sensitivity to radiation could be assessed by measuring liver perfusion during a course of treatment using dynamic contrast-enhanced computed tomography scanning.
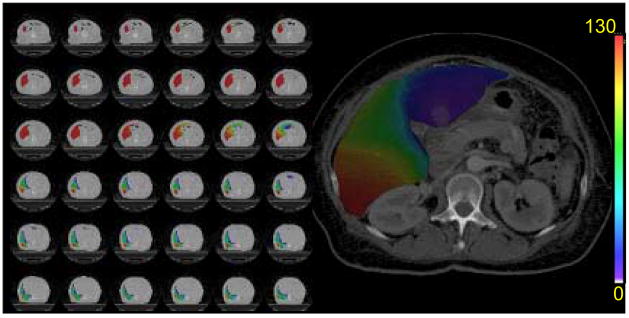
Methods and materials: Patients with intrahepatic cancer undergoing conformal radiotherapy underwent dynamic contrast-enhanced computed tomography (to measure perfusion distribution) and an indocyanine extraction study (to measure liver function) before, during, and 1 month after treatment. We hoped to determine whether the residual functioning liver (i.e., those regions showing portal vein perfusion) could be used to predict overall liver function after irradiation.
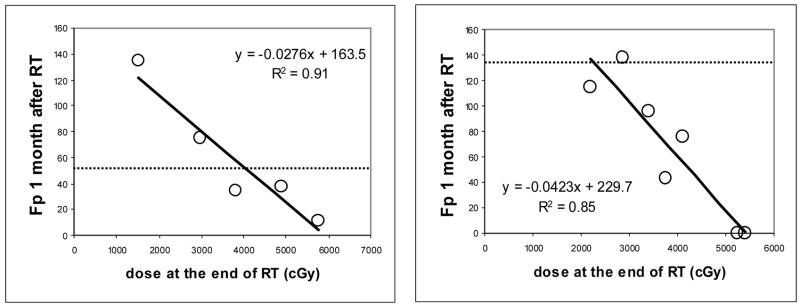
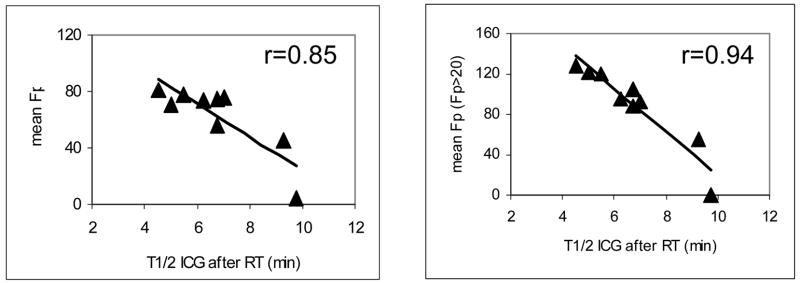
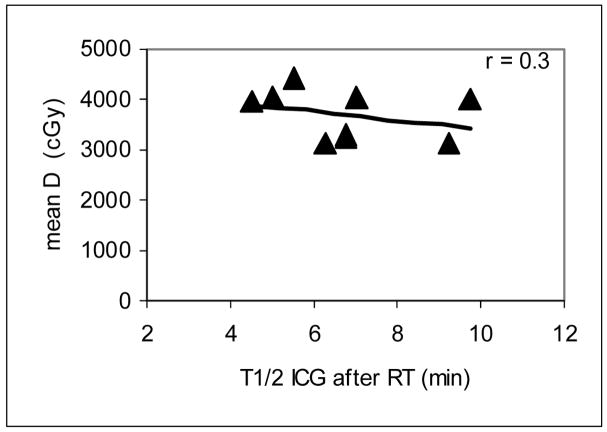
Results: Radiation doses from 45 to 84 Gy resulted in undetectable regional portal vein perfusion 1 month after treatment. The volume of each liver with undetectable portal vein perfusion ranged from 0 to 39% and depended both on the patient's sensitivity and on dose distribution. There was a significant correlation between indocyanine green clearance and the mean of the estimated portal vein perfusion in the functional liver parenchyma (p < 0.001).
Conclusion: This study reveals substantial individual variability in the sensitivity of the liver to irradiation. In addition, these findings suggest that hepatic perfusion imaging may be a marker for liver function and has the potential to be a tool for individualizing therapy.
Conflict of interest statement
Conflicts of Interest Notification:
None of authors has any actual or potential conflicts of interest related to this study.
Figures
References
-
- Ben-Josef E, Normolle D, Ensminger WD, et al. Phase II trial of high-dose conformal radiation therapy with concurrent hepatic artery floxuridine for unresectable intrahepatic malignancies. J Clin Oncol. 2005;23:8739–8747. - PubMed
-
- Emami B, Lyman J, Brown A, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys. 1991;21:109–122. - PubMed
-
- Lawrence TS, Robertson JM, Anscher MS, et al. Hepatic toxicity resulting from cancer treatment. Int J Radiat Oncol Biol Phys. 1995;31:1237–1248. - PubMed
-
- Gottlieb ME, Stratton HH, Newell JC, et al. Indocyanine green. Its use as an early indicator of hepatic dysfunction following injury in man. Arch Surg. 1984;119:264–268. - PubMed
-
- Hemming AW, Scudamore CH, Shackleton CR, et al. Indocyanine green clearance as a predictor of successful hepatic resection in cirrhotic patients. Am J Surg. 1992;163:515–518. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
