

Race and mortality after acute renal failure
- PMID: 17855647
- PMCID: PMC3023164
- DOI: 10.1681/ASN.2006091060
Race and mortality after acute renal failure
Abstract
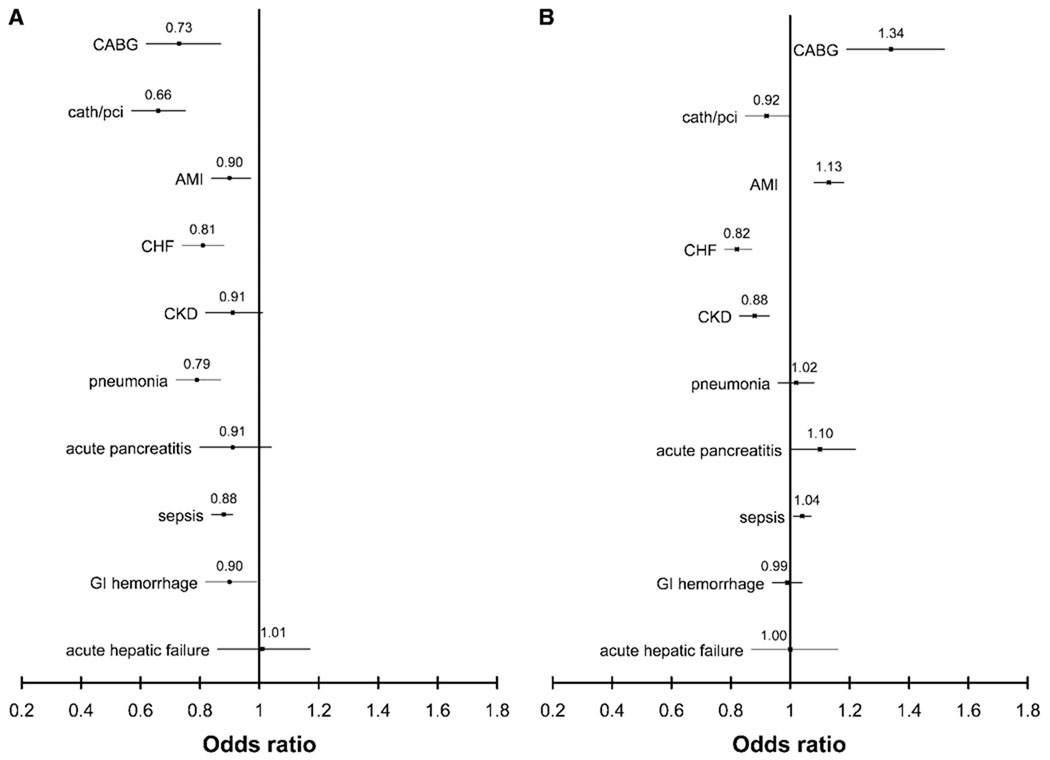
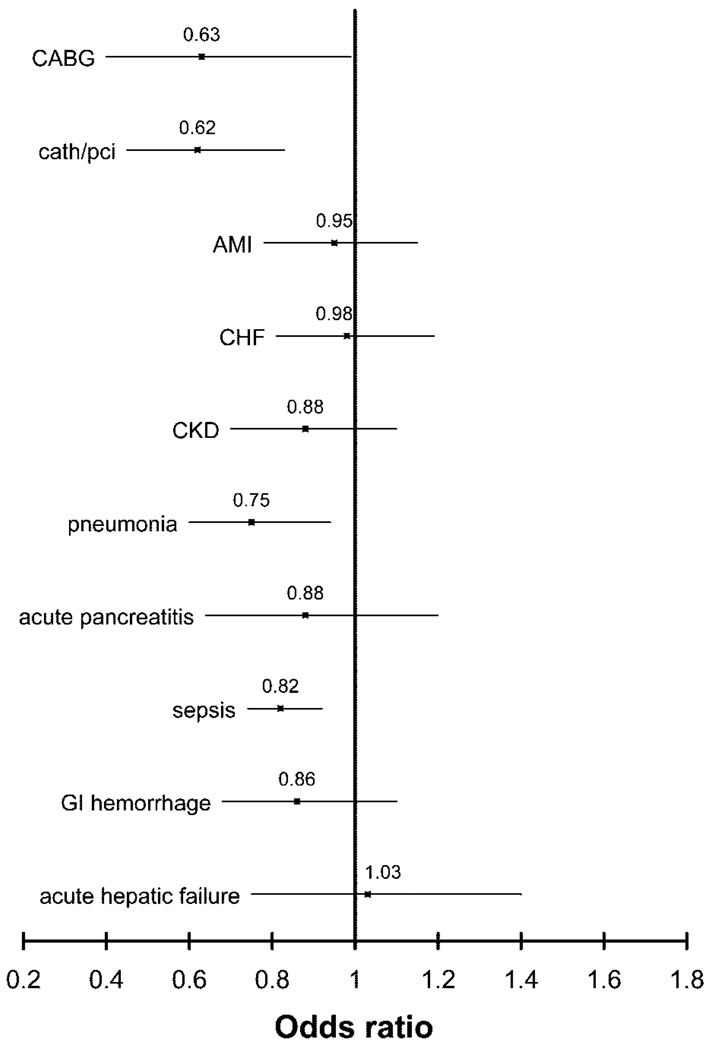
Black patients receiving dialysis for end-stage renal disease in the United States have lower mortality rates than white patients. Whether racial differences exist in mortality after acute renal failure is not known. We studied acute renal failure in patients hospitalized between 2000 and 2003 using the Nationwide Inpatient Sample and found that black patients had an 18% (95% confidence interval [CI] 16 to 21%) lower odds of death than white patients after adjusting for age, sex, comorbidity, and the need for mechanical ventilation. Similarly, among those with acute renal failure requiring dialysis, black patients had a 16% (95% CI 10 to 22%) lower odds of death than white patients. In stratified analyses of patients with acute renal failure, black patients had significantly lower adjusted odds of death than white patients in settings of coronary artery bypass grafting, cardiac catheterization, acute myocardial infarction, congestive heart failure, pneumonia, sepsis, and gastrointestinal hemorrhage. Black patients were more likely than white patients to be treated in hospitals that care for a larger number of patients with acute renal failure, and black patients had lower in-hospital mortality than white patients in all four quartiles of hospital volume. In conclusion, in-hospital mortality is lower for black patients with acute renal failure than white patients. Future studies should assess the reasons for this difference.
Figures
References
-
- Mortality patterns—United States, 1997. MMWR Morb Mortal Wkly Rep. 1999;48:664–668. - PubMed
-
- Vaccarino V, Rathore SS, Wenger NK, Frederick PD, Abramson JL, Barron HV, Manhapra A, Mallik S, Krumholz HM. National Registry of Myocardial Infarction Investigators: Sex and racial differences in the management of acute myocardial infarction, 1994 through 2002. N Engl J Med. 2005;353:671–682. - PMC - PubMed
-
- Peterson ED, Wright SM, Daley J, Thibault GE. Racial variation in cardiac procedure use and survival following acute myocardial infarction in the Department of Veterans Affairs. JAMA. 1994;271:1175–1180. - PubMed
-
- Burns RB, McCarthy EP, Freund KM, Marwill SL, Shwartz M, Ash A, Moskowitz MA. Black women receive less mammography even with similar use of primary care. Ann Intern Med. 1996;125:173–182. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
