

Low-tidal-volume ventilation in the acute respiratory distress syndrome
- PMID: 17855672
- PMCID: PMC2287190
- DOI: 10.1056/NEJMct074213
Low-tidal-volume ventilation in the acute respiratory distress syndrome
Abstract
A 55-year-old man who is 178 cm tall and weighs 95 kg is hospitalized with community-acquired pneumonia and progressively severe dyspnea. His arterial oxygen saturation while breathing 100% oxygen through a face mask is 76%; a chest radiograph shows diffuse alveolar infiltrates with air bronchograms. He is intubated and receives mechanical ventilation; ventilator settings include a tidal volume of 1000 ml, a positive end-expiratory pressure (PEEP) of 5 cm of water, and a fraction of inspired oxygen (FiO2) of 0.8. With these settings, peak airway pressure is 50 to 60 cm of water, plateau airway pressure is 38 cm of water, partial pressure of arterial oxygen is 120 mm Hg, partial pressure of carbon dioxide is 37 mm Hg, and arterial blood pH is 7.47. The diagnosis of the acute respiratory distress syndrome (ARDS) is made. An intensive care specialist evaluates the patient and recommends changing the current ventilator settings and implementing a low-tidal-volume ventilation strategy.
Figures
Comment in
-
Low-tidal-volume ventilation.N Engl J Med. 2007 Dec 13;357(24):2518-9; author reply 2519-20. doi: 10.1056/NEJMc072900. N Engl J Med. 2007. PMID: 18077819 No abstract available.
-
Low-tidal-volume ventilation.N Engl J Med. 2007 Dec 13;357(24):2519; author reply 2519-20. N Engl J Med. 2007. PMID: 18080385 No abstract available.
-
Low-tidal-volume ventilation.N Engl J Med. 2007 Dec 13;357(24):2519; author reply 2519-20. N Engl J Med. 2007. PMID: 18084817 No abstract available.
References
-
- Bernard GR, Artigas A, Brigham KL, et al. Report of the American-European Consensus Conference on acute respiratory distress syndrome: definitions, mechanisms, relevant outcomes, and clinical trial coordination. J Crit Care. 1994;9:72–81. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury. N Engl J Med. 2005;353:1685–93. - PubMed
-
- Piantadosi CA, Schwartz DA. The acute respiratory distress syndrome. Ann Intern Med. 2004;141:460–70. - PubMed
-
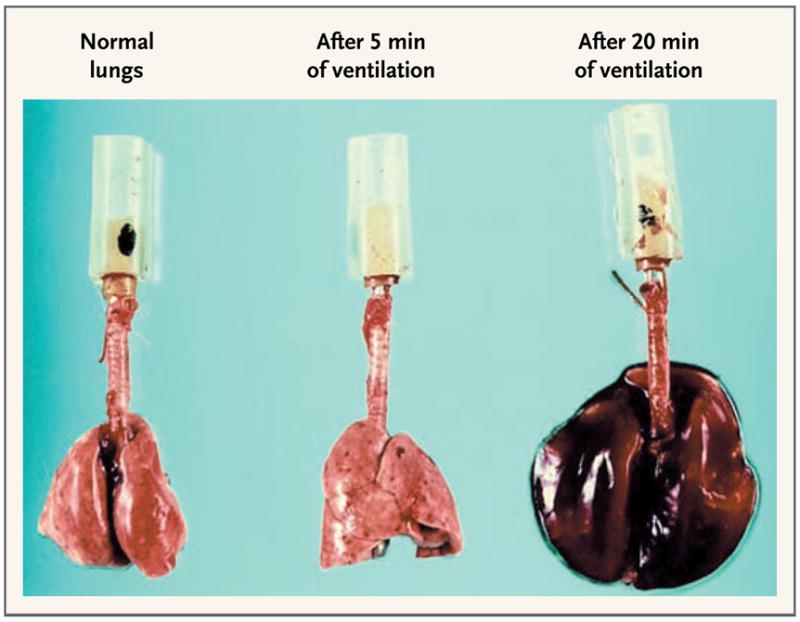
- Faridy EE, Permutt S, Riley RL. Effect of ventilation on surface forces in excised dogs’ lungs. J Appl Physiol. 1966;21:1453–62. - PubMed
-
- Spragg RG, Lewis JF, Walmrath H-D, et al. Effect of recombinant surfactant protein C–based surfactant on the acute respiratory distress syndrome. N Engl J Med. 2004;351:884–92. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical