

Enterococcal colonization of infants in a neonatal intensive care unit: associated predictors, risk factors and seasonal patterns
- PMID: 17868474
- PMCID: PMC2077867
- DOI: 10.1186/1471-2334-7-107
Enterococcal colonization of infants in a neonatal intensive care unit: associated predictors, risk factors and seasonal patterns
Abstract
Background: During and shortly after birth, newborn infants are colonized with enterococci. This study analyzes predictors for early enterococcal colonization of infants in a neonatal intensive care unit and describes risk factors associated with multidrugresistant enterococci colonization and its seasonal patterns.
Methods: Over a 12-month period, we performed a prospective epidemiological study in 274 infants admitted to a neonatal intensive care unit. On the first day of life, we compared infants with enterococcal isolates detected in meconium or body cultures to those without. We then tested the association of enterococcal colonization with peripartal predictors/risk factors by using bivariate and multivariate statistical methods.
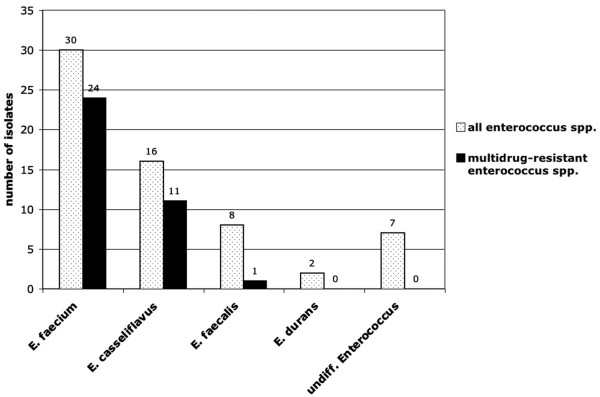
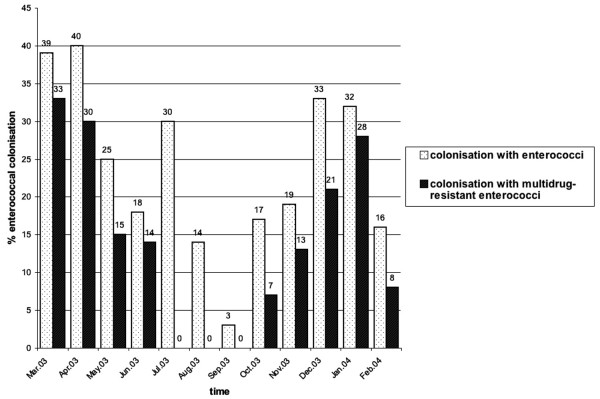
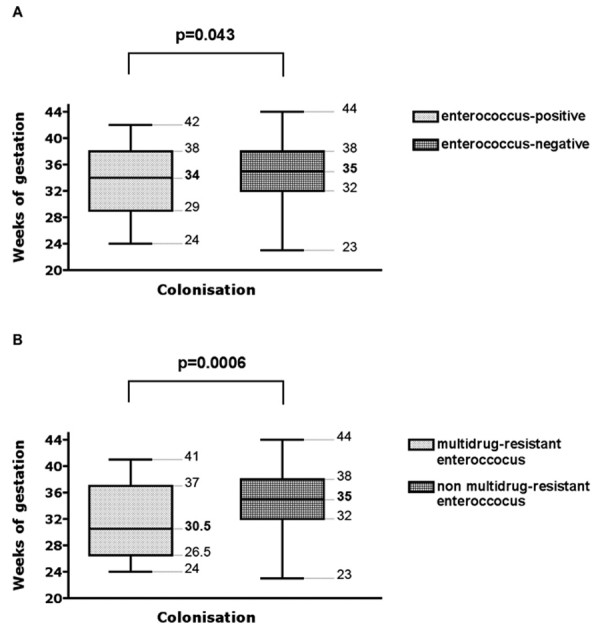
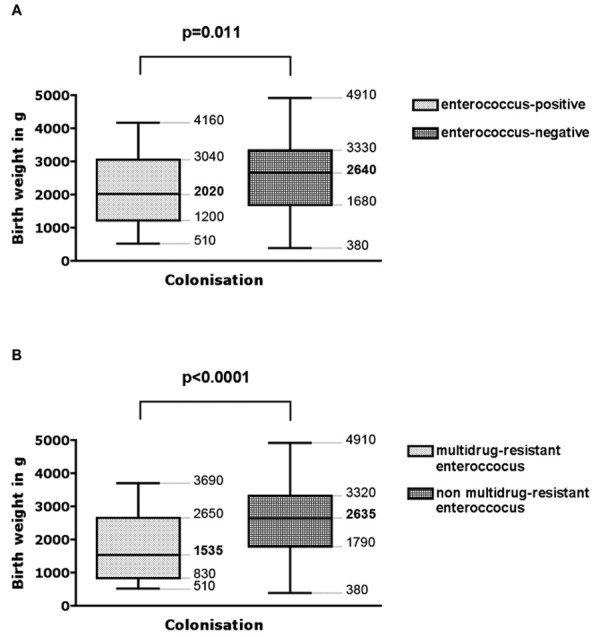
Results: Twenty-three percent of the infants were colonized with enterococci. The three most common enterococcal species were E. faecium (48% of isolates), E. casseliflavus (25%) and E. faecalis (13%). Fifty-seven percent of the enterococci found were resistant to three of five antibiotic classes, but no vancomycin-resistant isolates were observed. During winter/spring months, the number of enterococci and multidrug-resistant enterococci were higher than in summer/fall months (p = 0.002 and p < 0.0001, respectively). With respect to enterococcal colonization on the first day of life, predictors were prematurity (p = 0.043) and low birth weight (p = 0.011). With respect to colonization with multidrug-resistant enterococci, risk factors were prematurity (p = 0.0006), low birth weight (p < 0.0001) and prepartal antibiotic treatment (p = 0.019). Using logistic regression, we determined that gestational age was the only parameter significantly correlated with multidrug-resistant enterococci colonization. No infection with enterococci or multidrugresistant enterococci in the infants was detected. The outcome of infants with and without enterococcal colonization was the same with respect to death, necrotizing enterocolitis, intracerebral hemorrhage and bronchopulmonary dysplasia.
Conclusion: In neonatal intensive care units, an infant's susceptibility to early colonization with enterococci in general, and his or her risk for colonization with multidrug-resistant enterococci in particular, is increased in preterm newborns, especially during the winter/spring months. The prepartal use of antibiotics with no known activity against enterococci appears to increase the risk for colonization with multidrug-resistant enterococci.
Figures
References
-
- Fanaro S, Chierici R, Guerrini P, Vigi V. Intestinal microflora in early infancy: composition and development. Acta Paediatr Suppl. 2003;441:48–55. - PubMed
-
- Mackie RI, Sghir A, Gaskin HR. Developmental microbial ecology of the neonatal gastrointestinal tract. Am J Clin Nutr. 1999;69:1035S–45S. - PubMed
-
- Orrhage K, Nord CE. Factors controlling the bacterial colonization of the intestine in breastfed infants. Acta Paediatr Suppl. 1999;430:47–57. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
