

Retinal nerve fiber structure versus visual field function in patients with ischemic optic neuropathy. A test of a linear model
- PMID: 17870170
- PMCID: PMC2987576
- DOI: 10.1016/j.ophtha.2007.06.001
Retinal nerve fiber structure versus visual field function in patients with ischemic optic neuropathy. A test of a linear model
Abstract
Purpose: To test a linear model relating the regional loss in retinal nerve fiber (RNFL) thickness to the corresponding regional loss in sensitivity with data from patients with previous anterior ischemic optic neuropathy (AION).
Design: Case-control study.
Participants: Twenty-four individuals with AION and 20 with normal vision were tested. The time since the AION attack ranged from 5.2 months to more than 20.3 years (median, 2.95 years).
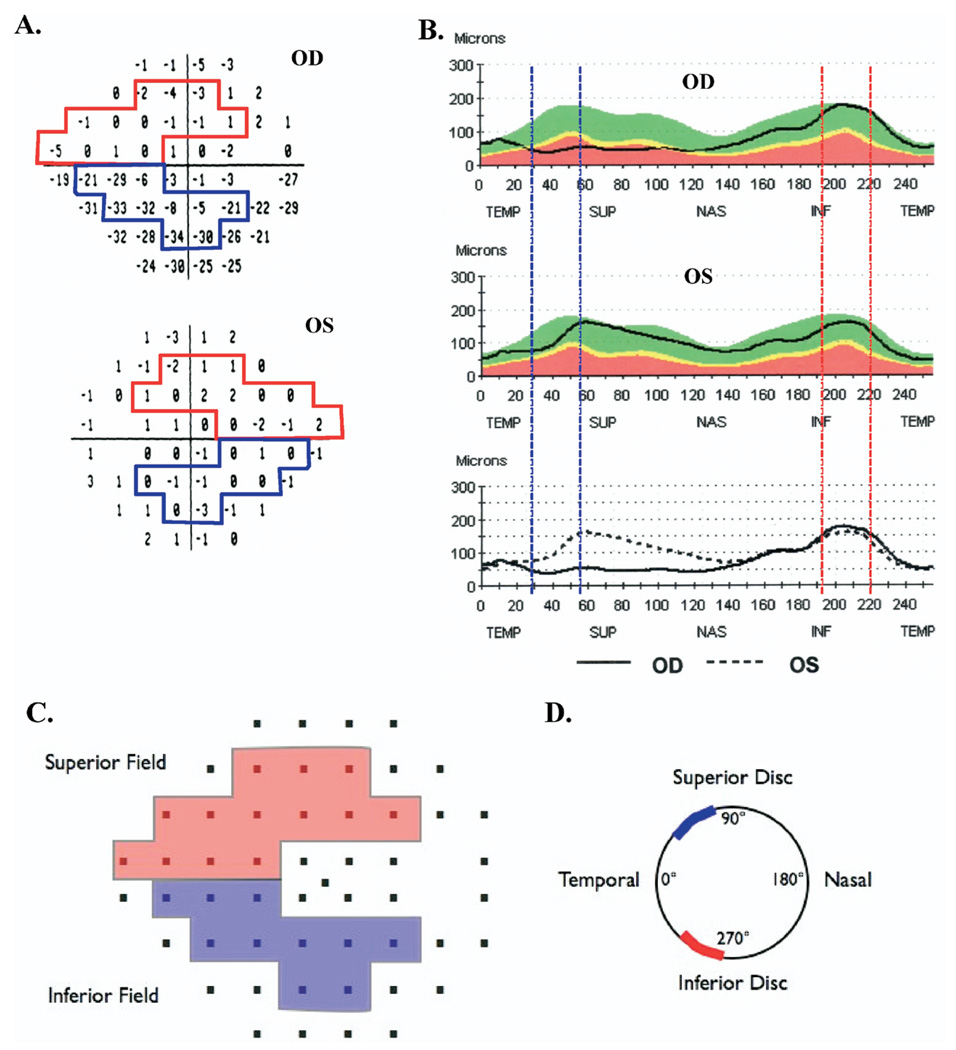
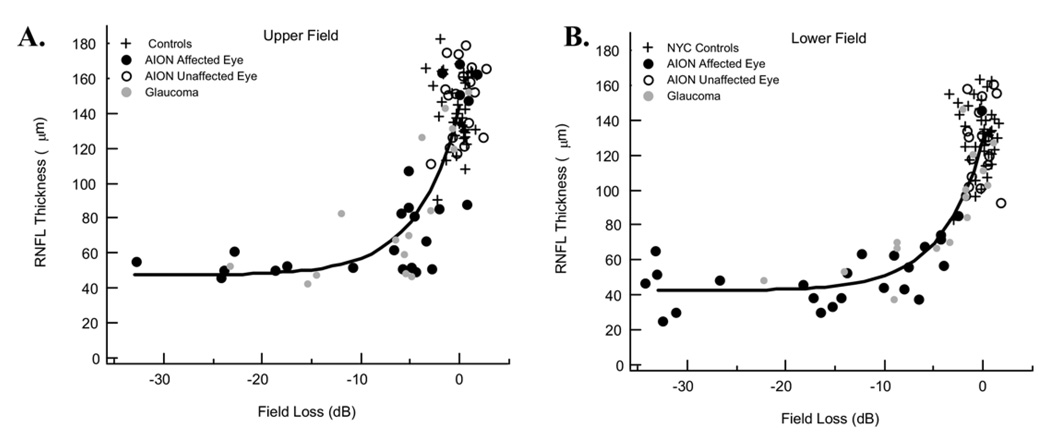
Methods: Eyes were tested with standard automated perimetry (SAP) and with optical coherence tomography (OCT), both RNFL thickness scans. The average RNFL thickness of the inferior and superior disc sectors was plotted against the average total deviations (linear units) of the corresponding superior and inferior arcuate field regions, and a linear model was fitted. According to the model, the RNFL thickness R=s(o)T+b, (1), where T is the relative SAP sensitivity loss (on a linear scale; e.g., for -3 dB, T = 0.5), s(o) is the RNFL thickness attributable to axons in the healthy or normal state (T = 1.0), and b is the residual RNFL measured when all sensitivity and axons are lost.
Main outcome measures: Optical coherence tomography RNFL thickness and SAP sensitivity.
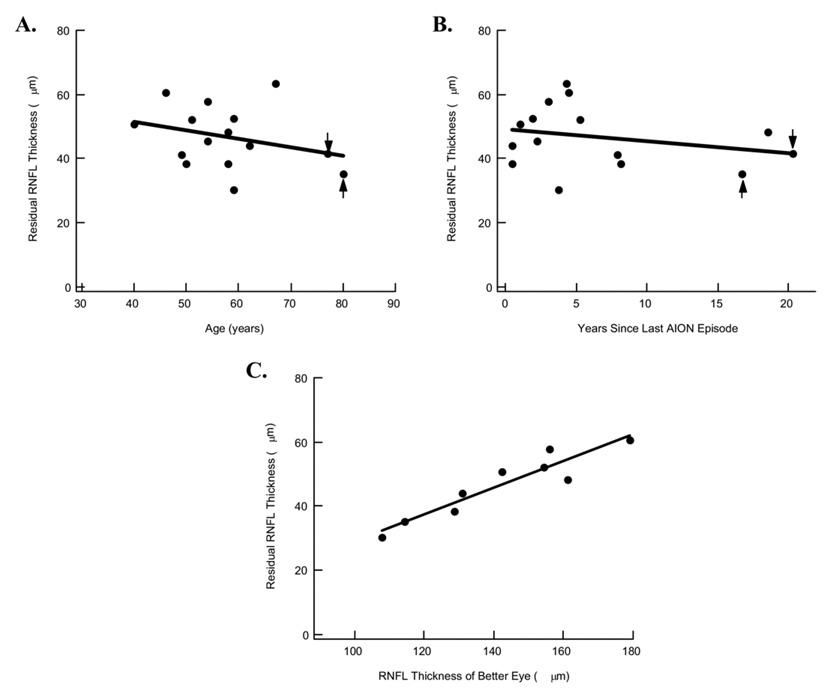
Results: The data from the AION patients resembled the data from glaucoma patients previously tested and were described by the linear model. For patients with SAP losses of more than -10 dB in the arcuate region, the RNFL thickness provided an estimate of residual RNFL thickness, b. The median value of b (45.5 microm) was similar to the value for patients with glaucoma. It varied among individuals (range, 30.4-63.3 microm), showing a very weak correlation with patient's age (r = 0.30) and the time since the AION episode (r = 0.26), but an excellent correlation (r(2) = 0.94; P<0.01) with the value of s(o), estimated from the unaffected eyes.
Conclusions: The relationship between a structure (OCT RNFL thickness) and function (SAP sensitivity loss) is the same for patients with AION and glaucoma and can be approximated by a simple linear model. The model may provide a framework for identifying those patients with ganglion cell axons that are malfunctioning but are alive.
Conflict of interest statement
The authors have no conflicts of interest related to the article.
Figures
References
-
- Garway-Heath DF. Comparison of structural and functional methods I. In: Weinreb RN, Greve EL, editors. Glaucoma Diagnosis: Structure and Function. Reports and Consensus Statements of the 1st Global AIGS Meeting on “Structure and Function in the Management of Glaucoma.”. The Hague: Kugler Publications; 2004. pp. 135–143.
-
- Garway-Heath DF, Holder GE, Fitzke FW, Hitchings RA. Relationship between electrophysiological, psychophysical, and anatomical measurements in glaucoma. Invest Ophthalmol Vis Sci. 2002;43:2213–2220. - PubMed
-
- Bowd C, Zangwill LM, Medeiros FA, et al. Structure-function relationships using confocal scanning laser ophthalmoscopy, optical coherence tomography, and scanning laser polarimetry. Invest Ophthalmol Vis Sci. 2006;47:2889–2895. - PubMed
-
- Swanson WH, Felius J, Pan F. Perimetric defects and ganglion cell damage: interpreting linear relations using a two-stage neural model. Invest Ophthalmol Vis Sci. 2004;45:466–472. - PubMed
-
- Hood DC, Greenstein VC, Odel JG, et al. Visual field defects and multifocal visual evoked potentials: evidence of a linear relationship. Arch Ophthalmol. 2002;120:1672–1681. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
