

Approach to diagnosis and management of abnormal uterine bleeding
- PMID: 17872610
- PMCID: PMC1952557
Approach to diagnosis and management of abnormal uterine bleeding
Abstract
Objective: To present a primary care approach to evaluating and managing abnormal uterine bleeding.
Sources of information: Literature searches were conducted on MEDLINE from 1996 to November 2004, EMBASE from 1996 to January 2005, the Cochrane Database of Systematic Reviews from the 4th quarter of 2004 to the 3rd quarter of 2005, guideline advisory committee databases, the Canadian Medical Association Infobase, and Clinical Evidence. The quality of evidence ranged from level I to III.
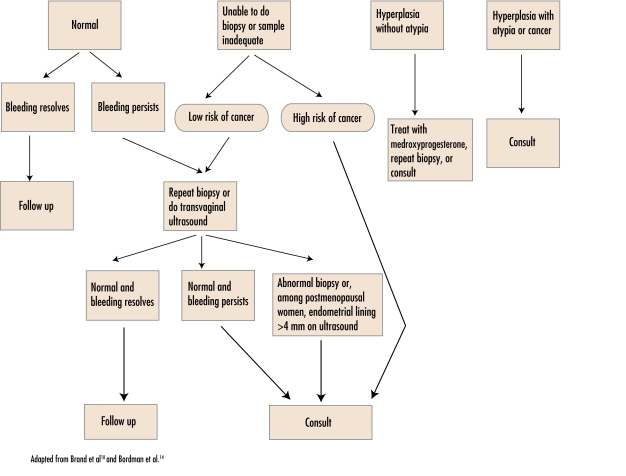
Main message: Premenopausal abnormal uterine bleeding can be ovulatory, anovulatory, or anatomic. A variety of hormonal and nonhormonal treatments are available. Patients' preferences, side effects, and physicians' comfort should be considered when making treatment decisions. One in 4 cases of endometrial carcinoma occur in premenopausal women, so it is important to investigate women with risk factors. While postmenopausal bleeding is most commonly caused by atrophic vaginitis, bleeding should be investigated to rule out endometrial and cervical carcinoma.
Conclusion: A primary care approach to medical management of abnormal uterine bleeding can help family physicians treat most women in the office as well as help physicians know when to refer women for specialist care.
OBJECTIF: Proposer une méthode adaptée aux soins primaires pour évaluer et traiter les saignements utérins anormaux.
SOURCES DE L’INFORMATION: On a consulté MEDLINE entre 1996 et novembre 2004, EMBASE entre 1996 et janvier 2005, la Cochrane Database of Systematic Reviews entre le 4e trimestre de 2004 et le 3e trimestre de 2005, des bases de données de comités consultatifs pour les directives de pratique, l’Infobasede l’Association médicale canadienne et Clinical Evidence. Les niveaux de preuves variaient entre I et III.
MESSAGE PRINCIPAL: Les saignements utérins anormaux peuvent être ovulatoires, anovulatoires ou anatomiques. Plusieurs traitements hormonaux ou non hormonaux sont disponibles. Le choix du traitement doit tenir compte des préférences de la patiente, des effets indésirables et des habitudes du médecin. Un quart des carcinomes endométriaux survient chez des femmes préménopausiques et il est donc important d’examiner celles qui présentent des facteurs de risque. Même si la plupart des saignements postménopausiques sont causés par la vaginite atrophique, ils méritent quand même d’être examinés pour éliminer un carcinome endométrial ou cervical.
CONCLUSION: Une méthode de traitement des saignements utérins anormaux adaptée aux soins primaires devrait aider le médecin de famille à traiter la plupart des femmes au bureau et lui permettre de savoir quand adresser la patiente en spécialité.
Figures
References
-
- O’Connor VM. Heavy menstrual loss. Part 1: Is it really heavy loss? Med Today. 2003;4(4):51–9.
-
- Vilos GA, Lefebvre G, Graves GR. Guidelines for the management of abnormal uterine bleeding. J Obstet Gynecol Can. 2001;23(8):704–9.
-
- Speroff L, Glass RH, Kase NG. Clinical gynecologic endocrinology and infertility. 6. Baltimore, Md: Lipincott Williams & Wilkins; 1999.
-
- Farquhar C, Ekeroma A, Fentiman G, Lethaby A, Rademaker L. An evidence-based guideline for the management of uterine fibroids. Aust N Z J Obstet Gynecol. 2001;41(2):125–40. - PubMed
-
- Reid RL, Lee JY. Medical management of menorrhagia. Informed. 1995;1(4):6–7.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials