

Approach to managing undiagnosed chest pain: could gastroesophageal reflux disease be the cause?
- PMID: 17872643
- PMCID: PMC1949125
Approach to managing undiagnosed chest pain: could gastroesophageal reflux disease be the cause?
Erratum in
- Can Fam Physician. 2007 Jul;53(7):1148
Abstract
Objective: To highlight gastroesophageal reflux disease as a common cause of undiagnosed chest pain.
Sources of information: Diagnostic considerations are based on information in peer-reviewed articles retrieved from MEDLINE. Studies had to be in English and involve at least 30 subjects. Population-based studies had to have a sample size of at least 300 and a response rate of at least 60%. Thirty-seven relevant articles were found.
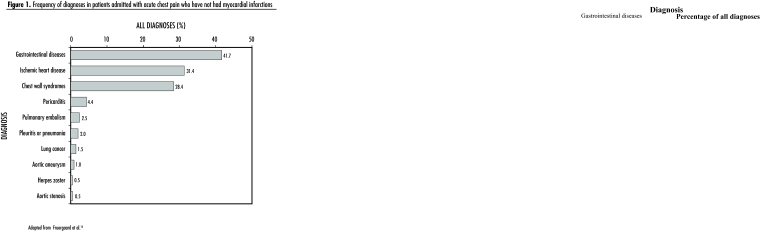
Main message: Clinical management of patients presenting with diagnostically challenging chest pain starts with a careful search for coronary artery disease and other potentially life-threatening causes. Investigations must continue until the underlying disease is identified and symptoms have been effectively controlled. Ongoing symptoms of undiagnosed chest pain cause considerable suffering, impair quality of life, and add unnecessary costs to the health care system. In more than half the patients with undiagnosed chest pain, symptoms are caused by gastroesophageal disease. Empirical acid-suppressive therapy with a proton pump inhibitor can assist clinicians in identifying patients whose symptoms are acid-related.
Conclusion: Many patients with undiagnosed chest pain can be managed in primary care, minimizing the need for referrals and costly investigations.
OBJECTIF: Mettre en évidence que le reflux gastro-œsophagien est une cause fréquente de douleur thoracique d’étiologie indéterminée.
SOURCES DE L’INFORMATION: Les considérations d’ordre diagnostique proviennent d’articles révisés par des pairs recensés dans MEDLINE. Les études devaient être en anglais et porter sur au moins 30 sujets. Dans les études démographiques, la taille des échantillons devait être d’au moins 300 et le taux de réponse d’au moins 60%. Trente-sept articles pertinents ont été retenus.
PRINCIPAL MESSAGE: Chez un patient qui présente une douleur thoracique d’origine incertaine, on doit d’abord rechercher soigneusement une maladie coronarienne ou toute autre cause potentielle de mort. L’investigation doit se poursuivre jusqu’à ce qu’on ait identifié la maladie causale et obtenu un contrôle adéquat des symptômes. Des douleurs thoraciques d’étiologieindéterminée entraînent à la longue d’importantes souffrances, une perte de qualité de vie et des coûts inutiles pour le système de santé. Dans plus de la moitié des cas de douleur thoracique non diagnostiquée, les symptômes sont causés par le reflux gastro-œsophagien. Un traitement empirique d’inhibition de la sécrétion acide par un inhibiteur de la pompe à protons peut aider le médecin à identifier les patients dont les symptômes sont reliés à l’acidité.
CONCLUSION: Plusieurs patients présentant des douleurs thoraciques d’origine indéterminée peuvent être traités adéquatement en soins de première ligne, réduisant ainsi le recours à des consultations ou investigations coûteuses.
Figures
Comment in
-
Chest pain--consider panic disorder.Can Fam Physician. 2007 May;53(5):807-8; author reply 808. Can Fam Physician. 2007. PMID: 17872738 Free PMC article. No abstract available.
-
Competing interests?Can Fam Physician. 2007 Jul;53(7):1146-7; author reply 1147; discussion 1147. Can Fam Physician. 2007. PMID: 17872805 Free PMC article. No abstract available.
References
-
- Ebell MH, Siwek J, Weiss BD, Woolf SH, Susman J, Ewigman B, et al. Strength of recommendation taxonomy (SORT): a patient-centered approach to grading evidence in the medical literature. Am Fam Physician. 2004;69(3):548–56. - PubMed
-
- Eslick GD, Jones MP, Talley NJ. Non-cardiac chest pain: prevalence, risk factors, impact and consulting—a population-based study. Aliment Pharmacol Ther. 2003;17(9):1115–24. - PubMed
-
- Brattberg G, Parker MG, Thorslund M. A longitudinal study of pain: reported pain from middle age to old age. Clin J Pain. 1997;13(2):144–9. - PubMed
-
- Locke GR, III, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ., III Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112(5):1448–56. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials