

Approach to managing musculoskeletal pain: acetaminophen, cyclooxygenase-2 inhibitors, or traditional NSAIDs?
- PMID: 17872814
- PMCID: PMC1949301
Approach to managing musculoskeletal pain: acetaminophen, cyclooxygenase-2 inhibitors, or traditional NSAIDs?
Abstract
Objective: To provide family physicians and pharmacists with practical, evidence- and expertise-based guidance on choosing the safest approach to using analgesics to manage patients with musculoskeletal pain.
Sources of information: Health care providers from family practice, rheumatology, gastroenterology, hepatology, internal medicine, and pharmacy participated in an educational needs assessment regarding the management of pain and the safety of commonly used analgesics. Feedback from one-on-one interviews was compiled and distributed to participants who selected key topics. Topics chosen formed the basis for the discussions of this multidisciplinary panel that reviewed data on the safety of analgesics, particularly in regard to comorbidity and concurrent use with other therapies.
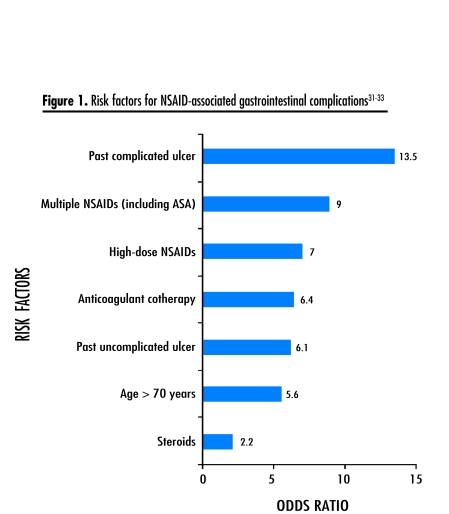
Main message: Treatment should begin with an effective analgesic with the best safety profile at the lowest dose and escalate to higher doses and different analgesics as required. Acetaminophen is a safe medication that should be considered first-line therapy. Nonsteroidal anti-inflammatory drugs (NSAIDs) are associated with potential adverse gastrointestinal, renal, hepatic, and cardiovascular effects. Physicians should not prescribe NSAIDs before taking a careful history and doing a physical examination so they have the information they need to weigh the risks (adverse effects and potential drug interactions) and benefits for individual patients.
Conclusion: Taking a complete and accurate history and doing a physical examination are essential for choosing the safest analgesic for a particular patient.
OBJECTIF: À partir de données probantes et d’opinions d’experts, fournir au médecin de famille et au pharmacien des directives sur la façon la plus sécuritaire d’utiliser les analgésiques pour traiter la douleur musculo-squelettique.
SOURCE DE L’INFORMATION: Divers membres du personnel soignant, médecins de famille, pharmaciens, spécialistes en rhumatologie, gastro-entérologie, hépatologie et médecine interne ont participé à une évaluation des besoins de formation sur le traitement de la douleur et l’innocuité des analgésiques d’usage courant. Les commentaires exprimés lors d’entrevues individuelles ont été compilés et distribués aux participants qui ont ensuite choisi les sujets les plus importants. Les sujets retenus ont alors été soumis pour discussion à ce groupe d’étude multidisciplinaire qui a fait une revue des données sur l’innocuité des analgésiques, notamment en relation avec la comorbidité et l’usage concomitant d’autres types de traitement.
PRINCIPAL MESSAGE: On devrait commencer par un analgésique efficace ayant le meilleur profil d’innocuité à la dose la plus faible et passer à des doses plus fortes ou à un autre analgésique si nécessaire. L’acétaminophène est un médicament sécuritaire qui devrait être envisagé comme traitement de première intention. Les anti-inflammatoires non stéroïdiens (AINS) sont susceptibles d’entraîner des effets indésirables aux niveaux gastrointestinal, rénal, hépatique et cardiovasculaire et le médecin ne devrait en prescrire qu’après une histoire et un examen physique complet de façon à posséder l’informationnécessaire pour en évaluer les avantages et risques (effets indésirables et possibilité d’interaction médicamenteuse) pour chaque patient.
CONCLUSION: Une histoire complète et précise et un examen physique sont requis pour choisir l’analgésique le plus sécuritaire pour un patient donné.
Figures
References
-
- Green LA, Phillips RL, Fryer GE. The nature of primary medical care. In: Jones R, Britten N, Culpepper L, Gass D, Grol R, Mant D, et al., editors. Oxford textbook of primary medical care. London, Engl: Oxford University Press; 2003. pp. 3–10.
-
- Mäntyselkä P, Kumpusalo E, Ahonen R, Kumpusalo A, Kauhanen J, Viinamäki H, et al. Pain as a reason to visit the doctor: a study in Finnish primary health care. Pain. 2001;89:175–80. - PubMed
-
- IMS Health Canada. Canadian disease and therapeutic index, March 2005. Norwalk, Conn: IMS Health; 2006.
-
- A.C. Nielsen MarketTrack. National drug+GB+MM, latest 52 weeks ending March 31, 2006. Markham, Ont: A.C. Nielsen Canada; 2006.
-
- Ofman JJ, MacLean CH, Straus WL, Morton SC, Berger ML, Roth EA, et al. Meta-analysis of dyspepsia and nonsteroidal anti-inflammatory drugs. Arthritis Rheum. 2003;49:508–18. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials