

Left ventricular dyssynchrony assessed by two three-dimensional imaging modalities: phase analysis of gated myocardial perfusion SPECT and tri-plane tissue Doppler imaging
- PMID: 17874098
- PMCID: PMC2121116
- DOI: 10.1007/s00259-007-0539-6
Left ventricular dyssynchrony assessed by two three-dimensional imaging modalities: phase analysis of gated myocardial perfusion SPECT and tri-plane tissue Doppler imaging
Abstract
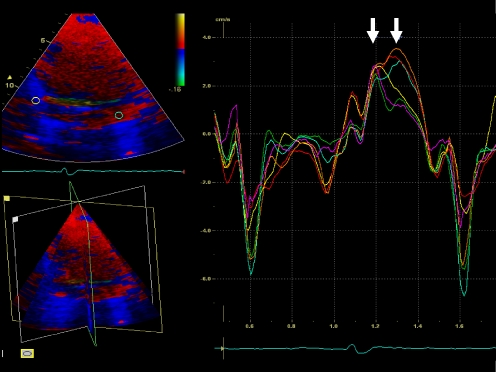
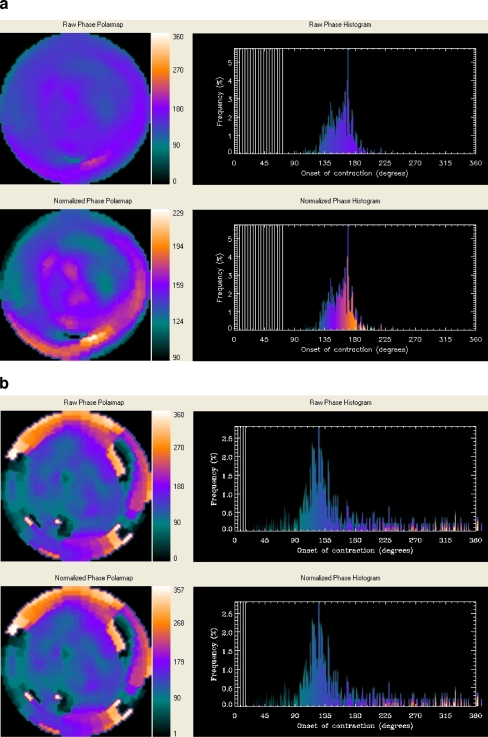
Purpose: To compare left ventricular (LV) dyssynchrony assessment by phase analysis from gated myocardial perfusion SPECT (GMPS) with LV dyssynchrony assessment by tri-plane tissue Doppler imaging (TDI). Baseline LV dyssynchrony assessed with standard deviation (SD) of time-to-peak systolic velocity of 12 LV segments (Ts-SD) with TDI has proven to be a powerful predictor of response to CRT. Information on LV dyssynchrony can also be provided by GMPS with phase analysis of regional LV maximal count changes throughout the cardiac cycle.
Methods: Forty heart failure patients, referred for evaluation of potential eligibility for CRT, underwent both 3D echocardiography, with tri-plane TDI, and resting GMPS. From tri-plane TDI, Ts-SD was used as a validated parameter of LV dyssynchrony and compared with different indices (histogram bandwidth, phase SD, histogram skewness and kurtosis) derived from phase analysis of GMPS.
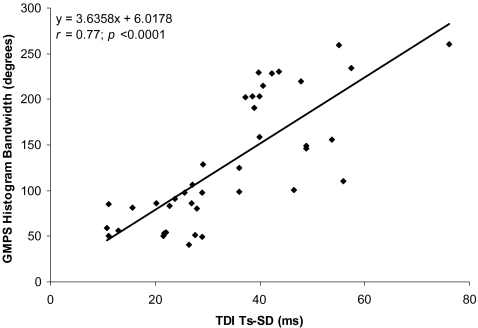
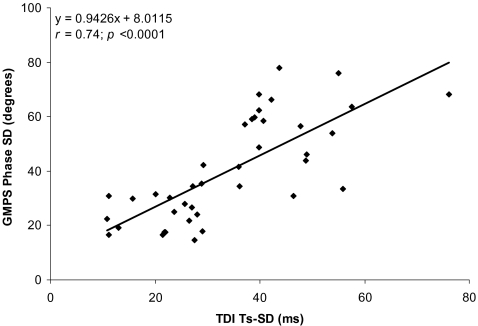
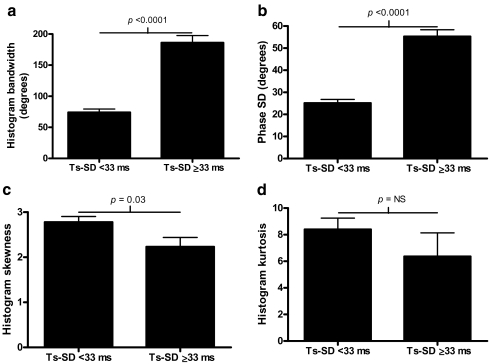
Results: Histogram bandwidth and phase SD showed good correlation with Ts-SD (r=0.77 and r=0.74, p<0.0001, respectively). Patients with substantial LV dyssynchrony assessed with tri-plane TDI (Ts-SD >or=33 ms) had also significantly higher values of histogram bandwidth and phase SD.
Conclusions: The results of this study support the use of phase analysis by GMPS to evaluate LV dyssynchrony. Histogram bandwidth and phase SD showed the best correlation with Ts-SD assessed with tri-plane TDI and appeared the most optimal variables for assessment of LV dyssynchrony with GMPS.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
