

Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): a diagnostic meta-analysis
- PMID: 17874169
- PMCID: PMC2219806
- DOI: 10.1007/s11606-007-0333-y
Screening for depression in medical settings with the Patient Health Questionnaire (PHQ): a diagnostic meta-analysis
Abstract
Objective: To summarize the psychometric properties of the PHQ2 and PHQ9 as screening instruments for depression.
Interventions: We identified 17 validation studies conducted in primary care; medical outpatients; and specialist medical services (cardiology, gynecology, stroke, dermatology, head injury, and otolaryngology). Electronic databases from 1994 to February 2007 (MEDLINE, PsycLIT, EMBASE, CINAHL, Cochrane registers) plus study reference lists have been used for this study. Translations included US English, Dutch, Italian, Spanish, German and Arabic). Summary sensitivity, specificity, likelihood and diagnostic odds ratios (OR) against a gold standard (DSM-IV) Major Depressive Disorder (MDD) were calculated for each study. We used random effects bivariate meta-analysis at recommended cut points to produce summary receiver-operator characteristic (sROC) curves. We explored heterogeneity with metaregression.
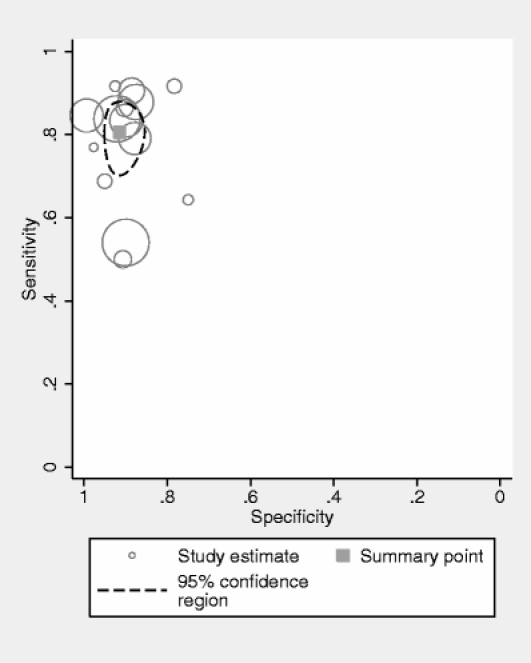
Measurements and main results: Fourteen studies (5,026 participants) validated the PHQ9 against MDD: sensitivity = 0.80 (95% CI 0.71-0.87); specificity = 0.92 (95% CI 0.88-0.95); positive likelihood ratio = 10.12 (95% CI 6.52-15.67); negative likelihood ratio = 0.22 (0.15 to 0.32). There was substantial heterogeneity (Diagnostic Odds Ratio heterogeneity I2 = 82%), which was not explained by study setting (primary care versus general hospital); method of scoring (cutoff > or = 10 versus "diagnostic algorithm"); or study quality (blinded versus unblinded). The diagnostic validity of the PHQ2 was only validated in 3 studies and showed wide variability in sensitivity.
Conclusions: The PHQ9 is acceptable, and as good as longer clinician-administered instruments in a range of settings, countries, and populations. More research is needed to validate the PHQ2 to see if its diagnostic properties approach those of the PHQ9.
Figures
References
-
- Pignone MP, Gaynes BN, Rushton JL, et al. Screening for depression in adults: a summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;136:765–76. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
