

Toll-like receptors in tumor immunotherapy
- PMID: 17875756
- PMCID: PMC2131730
- DOI: 10.1158/1078-0432.CCR-07-1378
Toll-like receptors in tumor immunotherapy
Abstract
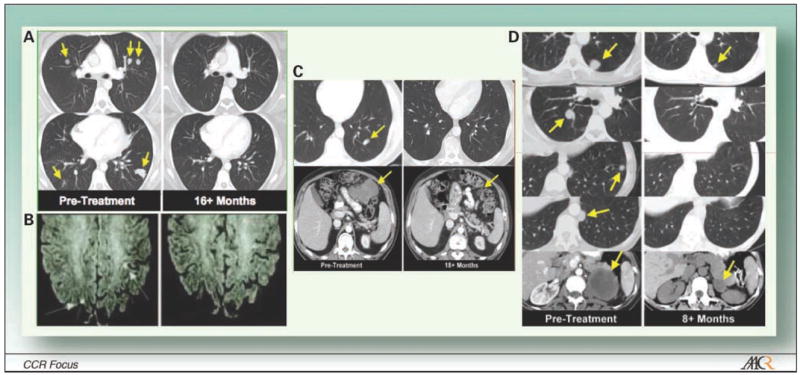
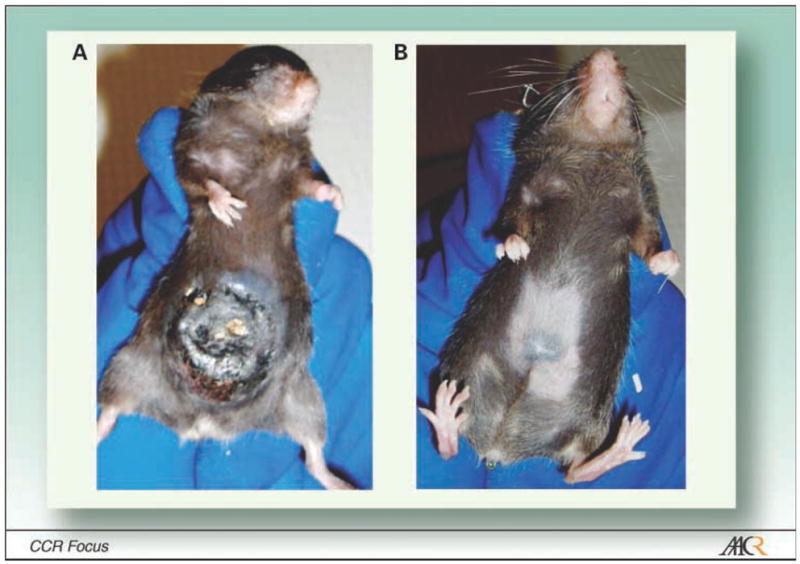
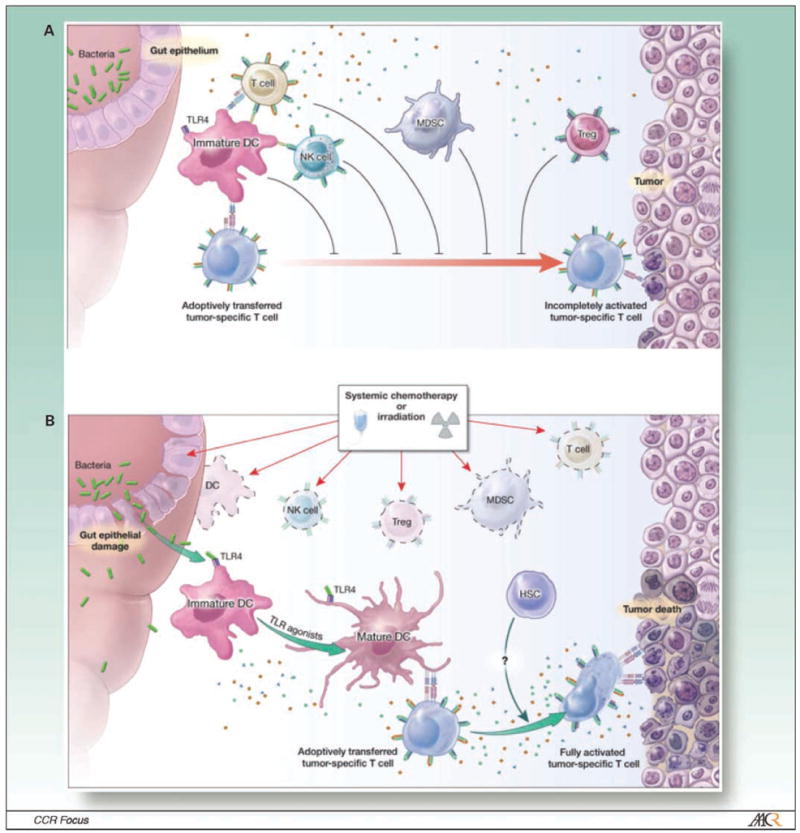
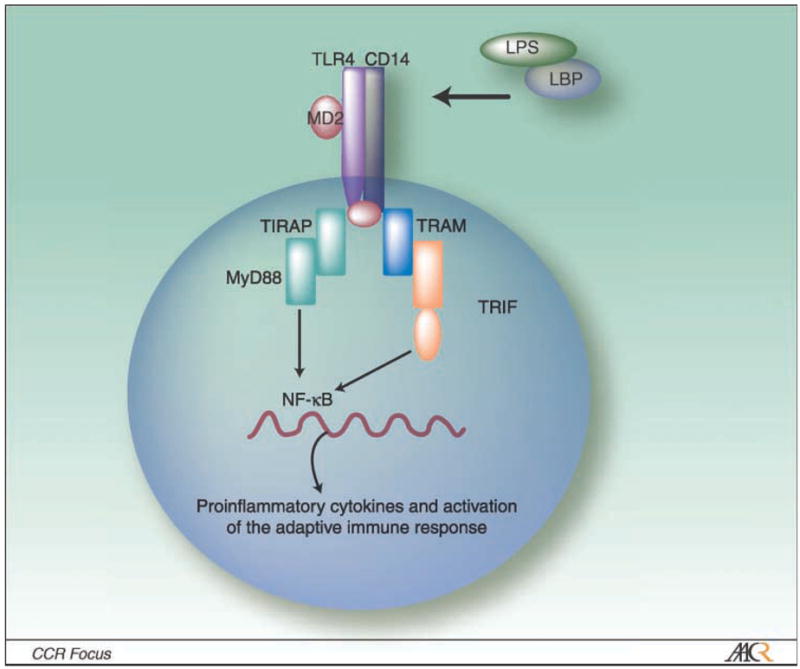
Lymphodepletion with chemotherapeutic agents or total body irradiation (TBI) before adoptive transfer of tumor-specific T cells is a critical advancement in the treatment of patients with melanoma. More than 50% of patients that are refractory to other treatments experience an objective or curative response with this approach. Emerging data indicate that the key mechanisms underlying how TBI augments the functions of adoptively transferred T cells include (a) the depletion of regulatory T cells (T(reg)) and myeloid-derived suppressor cells that limit the function and proliferation of adoptively transferred cells; (b) the removal of immune cells that act as "sinks" for homeostatic cytokines, whose levels increase after lymphodepletion; and (c) the activation of the innate immune system via Toll-like receptor 4 signaling, which is engaged by microbial lipopolysaccharide that translocated across the radiation-injured gut. Here, we review these mechanisms and focus on the effect of Toll-like receptor agonists in adoptive immunotherapy. We also discuss alternate regimens to chemotherapy or TBI, which might be used to safely treat patients with advanced disease and promote tumor regression.
Figures
References
-
- Coley WB. The treatment of malignant tumors by repeated inoculations of erysipelas. With a report of ten original cases.1893. Clin Orthop Relat Res. 1991:3–11. - PubMed
-
- Starnes CO. Coley’s toxins in perspective. Nature. 1992;357:11–2. - PubMed
-
- Matzinger P. The danger model: a renewed sense of self. Science. 2002;296:301–5. - PubMed
-
- Matzinger P. Tolerance, danger, and the extended family. Annu Rev Immunol. 1994;12:991–1045. - PubMed
-
- Medzhitov R, Janeway C., Jr The Toll receptor family and microbial recognition. Trends Microbiol. 2000;8:452–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
