

Severe acute pancreatitis: Clinical course and management
- PMID: 17876868
- PMCID: PMC4434632
- DOI: 10.3748/wjg.v13.i38.5043
Severe acute pancreatitis: Clinical course and management
Abstract
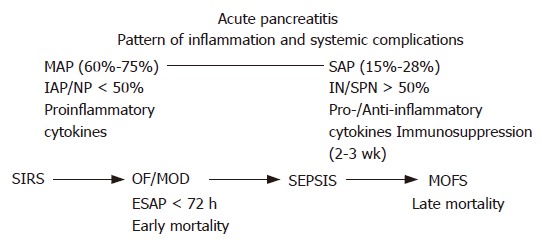
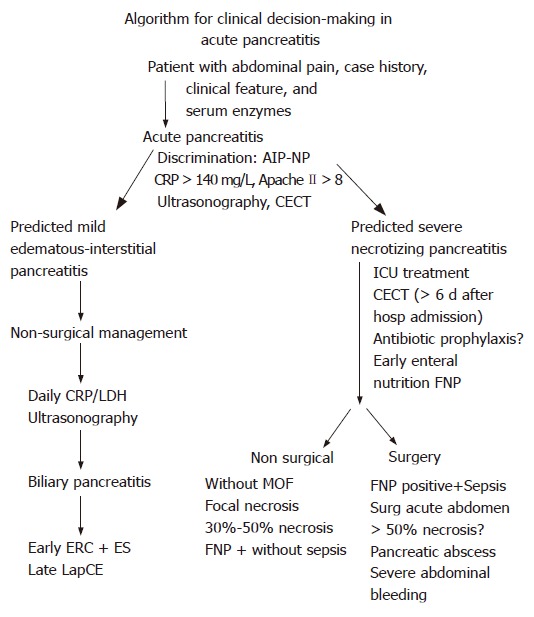
Severe acute pancreatitis (SAP) develops in about 25% of patients with acute pancreatitis (AP). Severity of AP is linked to the presence of systemic organ dysfunctions and/or necrotizing pancreatitis pathomorphologically. Risk factors determining independently the outcome of SAP are early multi-organ failure, infection of necrosis and extended necrosis (>50%). Up to one third of patients with necrotizing pancreatitis develop in the late course infection of necroses. Morbidity of SAP is biphasic, in the first week strongly related to early and persistence of organ or multi-organ dysfunction. Clinical sepsis caused by infected necrosis leading to multi-organ failure syndrome (MOFS) occurs in the later course after the first week. To predict sepsis, MOFS or deaths in the first 48-72 h, the highest predictive accuracy has been objectified for procalcitonin and IL-8; the Sepsis-Related Organ Failure Assessment (SOFA)-score predicts the outcome in the first 48 h, and provides a daily assessment of treatment response with a high positive predictive value. Contrast-enhanced CT provides the highest diagnostic accuracy for necrotizing pancreatitis when performed after the first week of disease. Patients who suffer early organ dysfunctions or at risk of developing a severe disease require early intensive care treatment. Early vigorous intravenous fluid replacement is of foremost importance. The goal is to decrease the hematocrit or restore normal cardiocirculatory functions. Antibiotic prophylaxis has not been shown as an effective preventive treatment. Early enteral feeding is based on a high level of evidence, resulting in a reduction of local and systemic infection. Patients suffering infected necrosis causing clinical sepsis, pancreatic abscess or surgical acute abdomen are candidates for early intervention. Hospital mortality of SAP after interventional or surgical debridement has decreased in high volume centers to below 20%.
Figures

References
-
- Dugernier TL, Laterre PF, Wittebole X, Roeseler J, Latinne D, Reynaert MS, Pugin J. Compartmentalization of the inflammatory response during acute pancreatitis: correlation with local and systemic complications. Am J Respir Crit Care Med. 2003;168:148–157. - PubMed
-
- Makhija R, Kingsnorth AN. Cytokine storm in acute pancreatitis. J Hepatobiliary Pancreat Surg. 2002;9:401–410. - PubMed
-
- Lipsett PA. Serum cytokines, proteins, and receptors in acute pancreatitis: mediators, markers, or more of the same? Crit Care Med. 2001;29:1642–1644. - PubMed
-
- Pezzilli R, Maldini M, Morselli-Labate AM, Barakat B, Romboli E, Beltrandi E, Migliori M, Tomassetti P, Corinaldesi R. Early activation of peripheral lymphocytes in human acute pancreatitis. J Clin Gastroenterol. 2003;36:360–363. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
