

Central nervous system capillary haemangioblastoma: the pathologist's viewpoint
- PMID: 17877533
- PMCID: PMC2517334
- DOI: 10.1111/j.1365-2613.2007.00535.x
Central nervous system capillary haemangioblastoma: the pathologist's viewpoint
Abstract
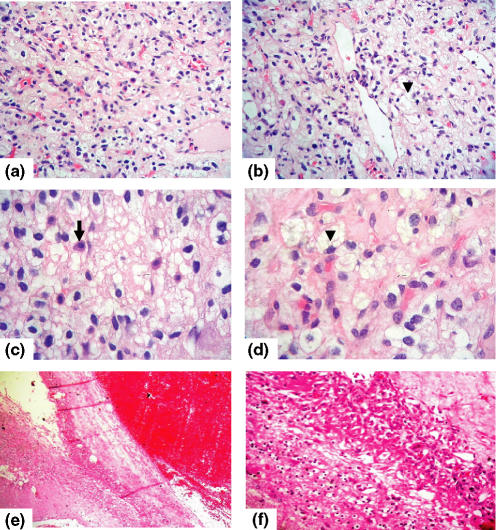
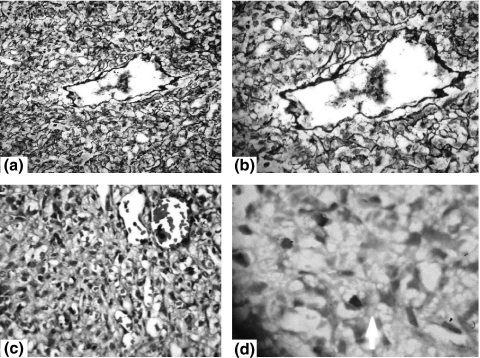
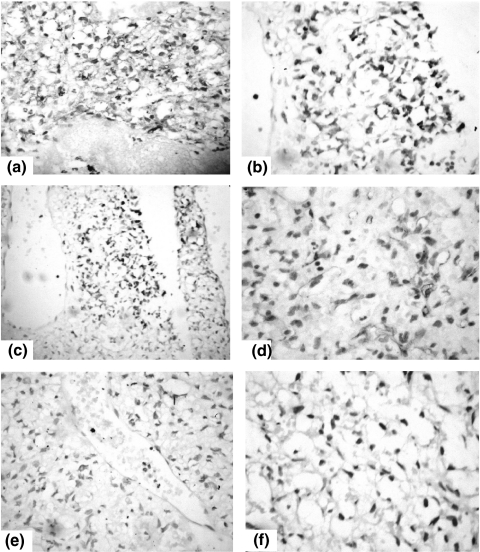
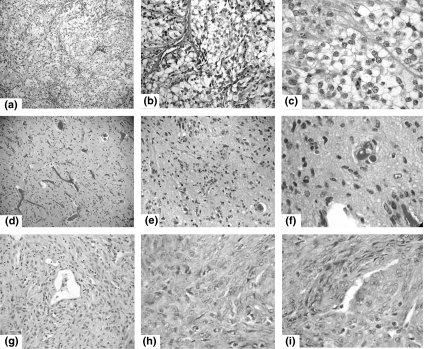
Haemangioblastomas are rare neoplasms of uncertain histogenesis. They represent 1.5-2.5% of intracranial tumours. While the cerebellum is by far the most frequent site, these lesions also tend to occur in the medulla and spinal cord. Most haemangioblastomas are sporadic but up to one quarter are associated with Von Hippel-Lindau disease (VHL). Although a fairly good number of haemangioblastomas were reported, a lack of side-by-side analysis of these reports has resulted in tentative conclusions that merely offer a first glimpse at their clinicopathologic diversity and histogenesis. To remedy this issue, this study presents a literature review concerning these lesions. Medline literature including both relevant monographs and clinicopathological case series. Haemangioblastomas occur either as a part of VHL disease (25-30%, inherited mutation of VHL gene on 3p25-26 chromosome) or as sporadic tumours (often with somatic mutation of VHL gene). They have diverse clinicopathologic presentations with cerebellar lesions having a better prognosis than their brainstem counterparts. Immunostaining is important for separation of haemangioblastomas from other tumours with similar histology. The rich vascularity of haemangioblastomas is due to overexpression of vascular endothelial growth factors. Moreover, 'stromal' cells represent the neoplastic cells of haemangioblastomas and are capable of forming blood islands with extramedullary haematopoiesis.
Figures
References
-
- Acikalin MF, Oner U, Tel N, Pasaoglu O, Altinel F. [Round table: infratentorial hemangioblastoma] Neurochirurgie. 1985;31:91–149. - PubMed
-
- Acikalin MF, Oner U, Tel N, Pasaoglu O, Altinel F. Supratentorial hemangioblastoma: a case report and review of the literature. Arch. Pathol. Lab. Med. 2003;127:e382–e384. - PubMed
-
- Altinoz MA, Santaguida C, Guiot MC, Del Maestro RF. Spinal hemangioblastoma containing metastatic renal cell carcinoma in von Hippel-Lindau disease. Case report and review of the literature. J. Neurosurg. Spine. 2005;3:495–500. - PubMed
-
- Arao T, Okada Y, Tanikawa T, et al. A case of von Hippel-Lindau disease with bilateral pheochromocytoma, renal cell carcinoma, pelvic tumor, spinal hemangioblastoma and primary hyperparathyroidism. Endocr. J. 2002;49:181–188. - PubMed
-
- Baccari P, Colombo R, Spotti D, Giovannelli M, Corlatti M, Staudacher C. Multidisciplinar surgical treatment in a case of von Hippel-Lindau with CNS hemangioblastoma, bilateral adrenal pheochromocytoma and multiple bilateral renal cell carcinoma – a case report. Contrib. Nephrol. 2001;136:281–283. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
