

Assessment of quality of life in HAART-treated HIV-positive subjects with body fat redistribution in Rwanda
- PMID: 17877798
- PMCID: PMC2075499
- DOI: 10.1186/1742-6405-4-19
Assessment of quality of life in HAART-treated HIV-positive subjects with body fat redistribution in Rwanda
Abstract
Background: The introduction of HAART has initially improved the quality of life (QoL) of HIV-positive (HIV+) patients, however body fat redistribution (BFR) and metabolic disorders associated with long-term HAART use may attenuate this improvement. As access to treatment improves in sub-Saharan Africa, the disfiguring nature of BFR (peripheral atrophy and/or central adiposity) may deter treatment adherence and initiatives and decrease QoL. We examined the relationship between BFR and domains of QoL in HAART-treated HIV+ African men and women with (HIV+BFR, n = 50) and without (HIV+noBFR, n = 50) BFR in Rwanda.
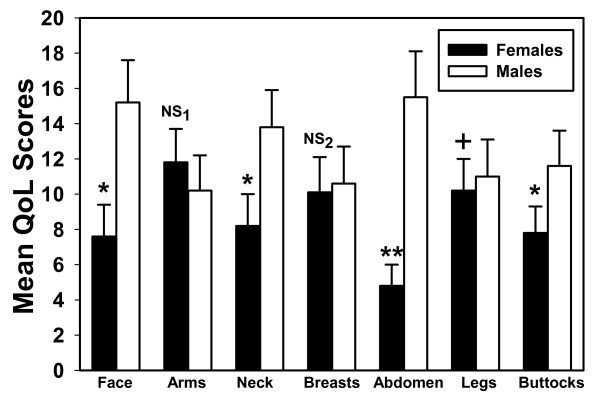
Results: HIV+ subjects with BFR were less satisfied with their body image (4.3 +/- 0.1 versus 1.5 +/- 0.2; p < .001), self-esteem and social life (4.1 +/- 1.4 versus 2.1 +/- 0.3; p = 0.003). HIV+BFR were more ashamed in public (4.5 +/- 1.2 versus 1.1 +/- 1.1), reported less confident about their health (4.6 +/- 1.4 versus 1.5 +/- 1.2) and were frequently embarrassed due to body changes (4.1 +/- 1.1 versus 1.1 +/- 0.9) (p < .001) than HIV+noBFR. HIV+ Rwandan women with BFR reported more dissatisfaction with psychological (8.3 +/- 2.9 versus 13.7 +/- 1.9), social relationships (6.9 +/- 2.3 versus 11.1 +/- 4.1) and HIV HAART-specific domain of wellbeing (3.1 +/- 4.8 versus 6.3 +/- 3.6) (p < .001). Age was associated with independence (r2 = 0.691; p = 0.009) and marital status was associated with psychological (r2 = 0.593; p = 0.019) and social relationships (r2 = 0.493; p = 0.007). CD4 count (r2 = 0.648; p = 0.003) and treatment duration (r2 = 0.453; p = 0.003) were associated with HIV HAART-specific domain of wellbeing. HIV+ Rwandan women with BFR were significantly more affected by abdominal adiposity (p < .001), facial and buttocks atrophy (p < .05) than HIV+ men with BFR.
Conclusion: Body fat alterations negatively affect psychological and social domains of quality of life. These symptoms may result in stigmatization and marginalization mainly in HAART-treated African women, adversely affecting HAART adherence and treatment initiatives. Efforts to evaluate self-perceived body fat changes may improve patients' wellbeing, HAART adherence and treatment outcomes and contribute towards stability in quality of life continuum.
Figures
Similar articles
-
The effects of exercise training on quality of life in HAART-treated HIV-positive Rwandan subjects with body fat redistribution.Qual Life Res. 2008 Apr;17(3):377-85. doi: 10.1007/s11136-008-9319-4. Epub 2008 Mar 5. Qual Life Res. 2008. PMID: 18320351 Free PMC article. Clinical Trial.
-
Exercise training reduces central adiposity and improves metabolic indices in HAART-treated HIV-positive subjects in Rwanda: a randomized controlled trial.AIDS Res Hum Retroviruses. 2008 Jan;24(1):15-23. doi: 10.1089/aid.2007.0023. AIDS Res Hum Retroviruses. 2008. PMID: 18275343 Free PMC article. Clinical Trial.
-
[Adherence to HAART, quality of life and psychopathological symptoms among HIV/AIDS infected patients].Acta Med Port. 2011 Dec;24 Suppl 2:539-48. Epub 2011 Dec 31. Acta Med Port. 2011. PMID: 22849945 Portuguese.
-
Lipodystrophy in the patient with HIV: social, psychological, and treatment considerations.Aesthet Surg J. 2008 Jul-Aug;28(4):443-51. doi: 10.1016/j.asj.2008.04.009. Aesthet Surg J. 2008. PMID: 19083560 Review.
-
Study of the impact of HIV genotypic drug resistance testing on therapy efficacy.Verh K Acad Geneeskd Belg. 2001;63(5):447-73. Verh K Acad Geneeskd Belg. 2001. PMID: 11813503 Review.
Cited by
-
The physical and psychological effects of HIV infection and its treatment on perinatally HIV-infected children.J Int AIDS Soc. 2015 Dec 2;18(Suppl 6):20258. doi: 10.7448/IAS.18.7.20258. eCollection 2015. J Int AIDS Soc. 2015. PMID: 26639114 Free PMC article.
-
The human immunodeficiency virus and the cardiometabolic syndrome in the developing world: an African perspective.J Cardiometab Syndr. 2008 Spring;3(2):106-10. doi: 10.1111/j.1559-4572.2008.07584.x. J Cardiometab Syndr. 2008. PMID: 18453811 Free PMC article.
-
Longitudinal assessment of health related quality of life of HIV infected patients treated for tuberculosis and HIV in a high burden setting.Qual Life Res. 2016 Dec;25(12):3067-3076. doi: 10.1007/s11136-016-1332-4. Epub 2016 Jun 9. Qual Life Res. 2016. PMID: 27277213
-
Health-Related Quality of Life in HIV-Infected Men Who Have Sex with Men in China: A Cross-Sectional Study.Med Sci Monit. 2016 Aug 14;22:2859-70. doi: 10.12659/msm.897017. Med Sci Monit. 2016. PMID: 27522466 Free PMC article.
-
Getting to 90-90-90 in paediatric HIV: What is needed?J Int AIDS Soc. 2015 Dec 2;18(7Suppl 6):20770. doi: 10.7448/IAS.18.7.20770. eCollection 2015. J Int AIDS Soc. 2015. PMID: 28326130 Free PMC article. No abstract available.
References
-
- Sterne JA, Hernan MA, Ledergerber B, Tilling K, Weber R, Sendi P, Rickenbach M, Robins JM, Egger M, Swiss HIV Cohort Study Long-term effectiveness of potent antiretroviral therapy in preventing AIDS and death: a prospective cohort study. Lancet. 2005;366:378–384. doi: 10.1016/S0140-6736(05)67022-5. - DOI - PubMed
-
- Pujari SN, Dravid A, Naik E, Bhagat S, Tash K, Nadler JP, Sinnott JT. Lipodystrophy and dyslipidaemia among patients taking first-line, World Health Organisation-recommended highly active antiretroviral therapy regimens in Western India. J Acquir Immune Defic Syndr. 2005;39:199–202. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
