

Assessment of quality of life in HAART-treated HIV-positive subjects with body fat redistribution in Rwanda
- PMID: 17877798
- PMCID: PMC2075499
- DOI: 10.1186/1742-6405-4-19
Assessment of quality of life in HAART-treated HIV-positive subjects with body fat redistribution in Rwanda
Abstract
Background: The introduction of HAART has initially improved the quality of life (QoL) of HIV-positive (HIV+) patients, however body fat redistribution (BFR) and metabolic disorders associated with long-term HAART use may attenuate this improvement. As access to treatment improves in sub-Saharan Africa, the disfiguring nature of BFR (peripheral atrophy and/or central adiposity) may deter treatment adherence and initiatives and decrease QoL. We examined the relationship between BFR and domains of QoL in HAART-treated HIV+ African men and women with (HIV+BFR, n = 50) and without (HIV+noBFR, n = 50) BFR in Rwanda.
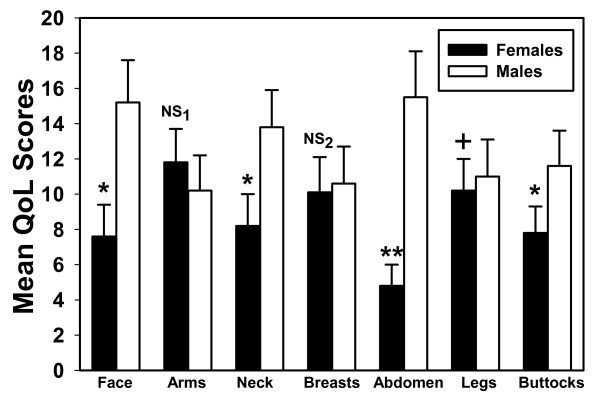
Results: HIV+ subjects with BFR were less satisfied with their body image (4.3 +/- 0.1 versus 1.5 +/- 0.2; p < .001), self-esteem and social life (4.1 +/- 1.4 versus 2.1 +/- 0.3; p = 0.003). HIV+BFR were more ashamed in public (4.5 +/- 1.2 versus 1.1 +/- 1.1), reported less confident about their health (4.6 +/- 1.4 versus 1.5 +/- 1.2) and were frequently embarrassed due to body changes (4.1 +/- 1.1 versus 1.1 +/- 0.9) (p < .001) than HIV+noBFR. HIV+ Rwandan women with BFR reported more dissatisfaction with psychological (8.3 +/- 2.9 versus 13.7 +/- 1.9), social relationships (6.9 +/- 2.3 versus 11.1 +/- 4.1) and HIV HAART-specific domain of wellbeing (3.1 +/- 4.8 versus 6.3 +/- 3.6) (p < .001). Age was associated with independence (r2 = 0.691; p = 0.009) and marital status was associated with psychological (r2 = 0.593; p = 0.019) and social relationships (r2 = 0.493; p = 0.007). CD4 count (r2 = 0.648; p = 0.003) and treatment duration (r2 = 0.453; p = 0.003) were associated with HIV HAART-specific domain of wellbeing. HIV+ Rwandan women with BFR were significantly more affected by abdominal adiposity (p < .001), facial and buttocks atrophy (p < .05) than HIV+ men with BFR.
Conclusion: Body fat alterations negatively affect psychological and social domains of quality of life. These symptoms may result in stigmatization and marginalization mainly in HAART-treated African women, adversely affecting HAART adherence and treatment initiatives. Efforts to evaluate self-perceived body fat changes may improve patients' wellbeing, HAART adherence and treatment outcomes and contribute towards stability in quality of life continuum.
Figures
References
-
- Sterne JA, Hernan MA, Ledergerber B, Tilling K, Weber R, Sendi P, Rickenbach M, Robins JM, Egger M, Swiss HIV Cohort Study Long-term effectiveness of potent antiretroviral therapy in preventing AIDS and death: a prospective cohort study. Lancet. 2005;366:378–384. doi: 10.1016/S0140-6736(05)67022-5. - DOI - PubMed
-
- Pujari SN, Dravid A, Naik E, Bhagat S, Tash K, Nadler JP, Sinnott JT. Lipodystrophy and dyslipidaemia among patients taking first-line, World Health Organisation-recommended highly active antiretroviral therapy regimens in Western India. J Acquir Immune Defic Syndr. 2005;39:199–202. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
