

Effectiveness and safety of chest pain assessment to prevent emergency admissions: ESCAPE cluster randomised trial
- PMID: 17878265
- PMCID: PMC1995498
- DOI: 10.1136/bmj.39325.624109.AE
Effectiveness and safety of chest pain assessment to prevent emergency admissions: ESCAPE cluster randomised trial
Abstract
Objective: To determine whether introducing chest pain unit care reduces emergency admissions without increasing reattendances and admissions over the next 30 days.
Design: Cluster randomised before and after intervention trial.
Setting: 14 diverse acute hospitals in the United Kingdom.
Participants: Patients attending the emergency department with acute chest pain during the year before and the year after the intervention started.
Intervention: Establishment of chest pain unit care compared with continuation of routine care.
Main outcome measures: Proportion of chest pain attendances resulting in admission; reattendances and admissions over the next 30 days; daily emergency medical admissions (all causes); and proportion of emergency department attendances with chest pain.
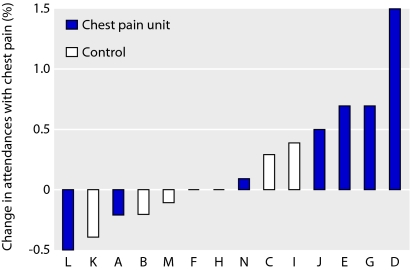
Results: The introduction of chest pain unit care was associated with weak evidence of an increase in emergency department attendances with chest pain (16% v 3.5%; P=0.08); no change in the proportion of chest pain attendances resulting in admission (odds ratio 0.998, 95% confidence interval 0.940 to 1.059; P=0.945); small increases in the proportion reattending (odds ratio 1.10, 1.00 to 1.21; P=0.036) or being admitted (1.30, 0.97 to 1.74; P=0.083) over the next 30 days; and evidence of increased daily medical admissions (1.7 per day, 95% confidence interval 0.8 to 2.5; P<0.001). However, this last finding was highly sensitive to changes in the method used to handle missing data.
Conclusion: The introduction of chest pain unit care did not reduce the proportion of patients with chest pain admitted and may have been associated with increased emergency department attendances with chest pain.
Trial registration: Current Controlled Trials ISRCTN55318418.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Effectiveness of chest pain units.BMJ. 2007 Sep 29;335(7621):623-4. doi: 10.1136/bmj.39339.380093.BE. BMJ. 2007. PMID: 17901470 Free PMC article.
References
-
- NHS Institute for Innovation and Improvement. Directory of emergency ambulatory care for adults Coventry: NHS Institute for Innovation and Improvement, 2007
-
- Roberts RR, Zalenski RJ, Mensah EK, Rydman RJ, Ciavarella G, Gussow L, et al. Costs of an emergency department-based accelerated diagnostic protocol vs hospitalization in patients with chest pain: a randomized controlled trial. JAMA 1997;278:1670-6. - PubMed
-
- Farkouh ME, Smars PA, Reeder GS, Zinsmeister AR, Evans RW, Meloy TD, et al. A clinical trial of a chest pain observation unit for patients with unstable angina. N Engl J Med 1998;339:1882-8. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical