

Pancreatic fistula after pancreaticoduodenectomy: a comparison between the two pancreaticojejunostomy methods for approximating the pancreatic parenchyma to the jejunal seromuscular layer: interrupted vs continuous stitches
- PMID: 17879405
- PMCID: PMC4171325
- DOI: 10.3748/wjg.v13.i40.5351
Pancreatic fistula after pancreaticoduodenectomy: a comparison between the two pancreaticojejunostomy methods for approximating the pancreatic parenchyma to the jejunal seromuscular layer: interrupted vs continuous stitches
Abstract
Aim: The purpose of this study is to find a better operative technique by comparing interrupted stitches with continuous stitches for the outer layer of the pancreaticojejunostomy, i.e. the stitches between the stump parenchyma of the pancreas and the jejunal seromuscular layer, and other risk factors for the incidence of pancreatic leakage.
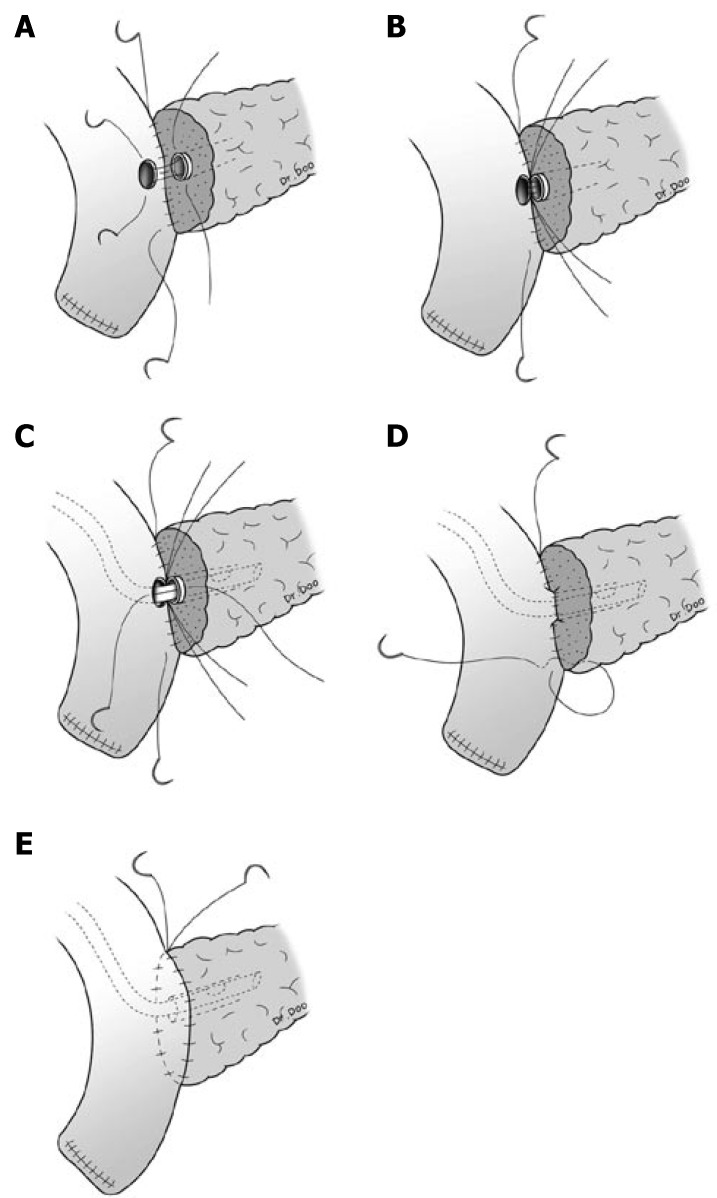
Methods: During the period January 1997 to October 2004, 133 patients have undergone the end-to-side and duct-to-mucosa pancreaticojejunostomy reconstruction after pancreaticoduodenectomy with interrupted suture for outer layer of the pancreaticojejunostomy and 170 patients with a continuous suture at our institution by one surgeon.
Results: There were no significant differences between the two groups in the diagnosis, texture of the pancreas, use of octreotide and pathologic stage. Pancreatic fistula occurred in 14 patients (11%) among the interrupted suture cases and in 10 (6%) among the continuous suture cases (P = 0.102). Major pancreatic leakage developed in three interrupted suture patients (2%) and zero continuous suture patients (P = 0.026). In multivariate analysis, soft pancreatic consistency (odds ratio, 5.5; 95% confidence interval 2.3-13.1) and common bile duct cancer (odds ratio, 3.7; 95% CI 1.6-8.5) were predictive of pancreatic leakage.
Conclusion: Pancreatic texture and pathology are the most important factors in determining the fate of pancreaticojejunal anastomosis and our continuous suture method was performed with significantly decreased occurrence of major pancreatic fistula. In conclusion, the continuous suture method is more feasible and safer in performing duct-to-mucosa pancreaticojejunostomy.
Figures
References
-
- Balcom JH, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg. 2001;136:391–398. - PubMed
-
- Bassi C, Falconi M, Salvia R, Mascetta G, Molinari E, Pederzoli P. Management of complications after pancreaticoduodenectomy in a high volume centre: results on 150 consecutive patients. Dig Surg. 2001;18:453–457; discussion 458. - PubMed
-
- van Berge Henegouwen MI, De Wit LT, Van Gulik TM, Obertop H, Gouma DJ. Incidence, risk factors, and treatment of pancreatic leakage after pancreaticoduodenectomy: drainage versus resection of the pancreatic remnant. J Am Coll Surg. 1997;185:18–24. - PubMed
-
- Yeh TS, Jan YY, Jeng LB, Hwang TL, Wang CS, Chen SC, Chao TC, Chen MF. Pancreaticojejunal anastomotic leak after pancreaticoduodenectomy--multivariate analysis of perioperative risk factors. J Surg Res. 1997;67:119–125. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
