

Review
doi: 10.3748/wjg.v13.i40.5391.
Sequential stenotic strictures of the small bowel leading to obstruction
Affiliations
- PMID: 17879413
- PMCID: PMC4171333
- DOI: 10.3748/wjg.v13.i40.5391
Item in Clipboard
Review
Sequential stenotic strictures of the small bowel leading to obstruction
World J Gastroenterol.
.
Abstract
Small bowel obstructions (SBOs) are primarily caused by adhesions, hernias, neoplasms, or inflammatory strictures. Intraluminal strictures are an uncommon cause of SBO. This report describes our findings in a unique case of sequential, stenotic intraluminal strictures of the small intestine, discusses the differential diagnosis of intraluminal intestinal strictures, and reviews the literature regarding intraluminal pathology.
Figures

CT scan of the abdomen. A CT scan of the abdomen revealed an SBO with dilation of small-intestinal loops, and a transition point in the mid-jejunum. A distended small was observed anteriorly of the air fluid level, and distal to this, a dilated loop and cross section was filled with feces, the so-called small bowel feces sign, which is indicative of SBO. Distal to the obstruction, there was a clear transition point in the mid-jejunum.
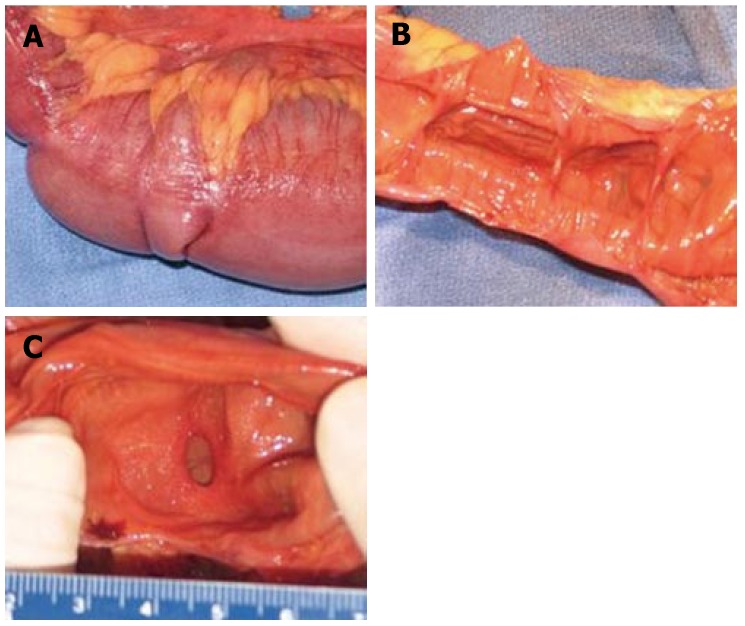
Gross specimens. Seventy-six centimeter segment of small intestine. On gross examination, fat surrounded the serosal surface of the intestine at irregular intervals, at the mesenteric border (A). Associated with these deposits of fat were 14 areas of mucosal stricture. In the normal intestine, the luminal diameter ranged from 4.7 to 9.5 cm. In the areas of luminal constriction, the diameter was 0.7 to 1.0 cm (B, C).
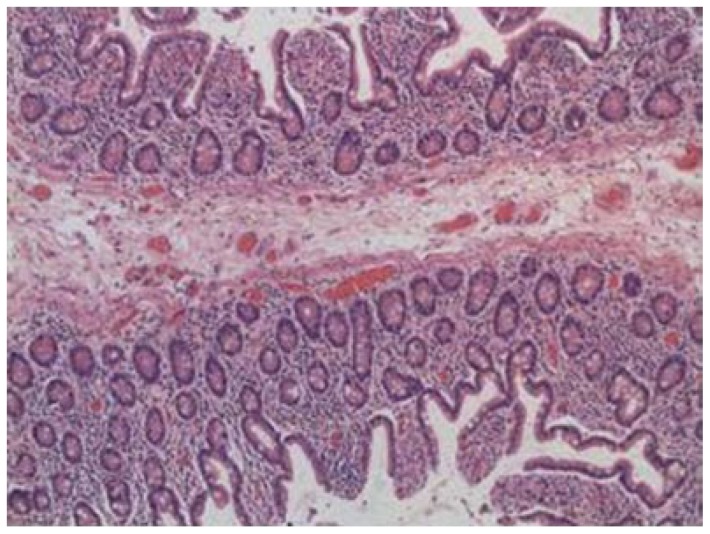
Microscopic image. On microscopic examination, the intestinal webs contained mucosa and submucosa. Muscularis propria was not present within the webs. There was no evidence of inflammatory bowel disease, malignancy, or pathologic inflammation of the bowel or mesentery.
References
-
- Nagle A, Ujiki M, Denham W, Murayama K. Laparoscopic adhesiolysis for small bowel obstruction. Am J Surg. 2004;187:464–470. - PubMed
-
- Dalla Vecchia LK, Grosfeld JL, West KW, Rescorla FJ, Scherer LR, Engum SA. Intestinal atresia and stenosis: a 25-year experience with 277 cases. Arch Surg. 1998;133:490–496; discussion 496-497. - PubMed
-
- Peetsold MG, Ekkelkamp S, Heij HA. Late presentation of a duodenal web in a patient with situs inversus and apple peel jejunal atresia. Pediatr Surg Int. 2004;20:301–303. - PubMed
-
- Hurst RD, Molinari M, Chung TP, Rubin M, Michelassi F. Prospective study of the features, indications, and surgical treatment in 513 consecutive patients affected by Crohn's disease. Surgery. 1997;122:661–667; discussion 667-668. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
