

Clindamycin-induced acute cholestatic hepatitis
- PMID: 17879418
- PMCID: PMC4171338
- DOI: 10.3748/wjg.v13.i40.5408
Clindamycin-induced acute cholestatic hepatitis
Abstract
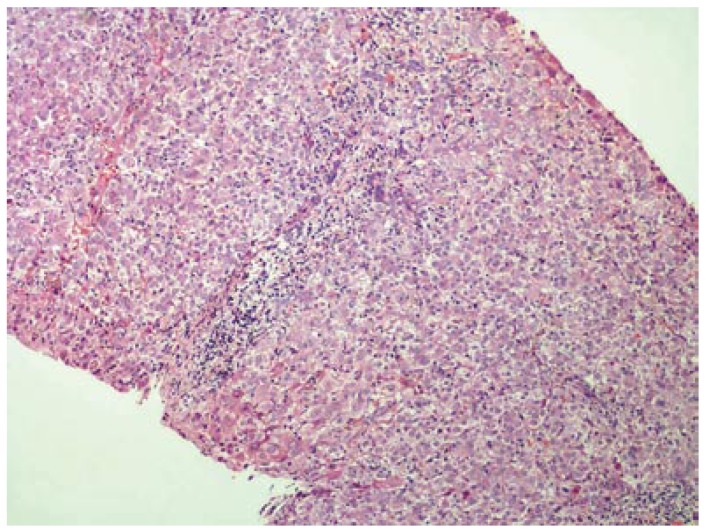
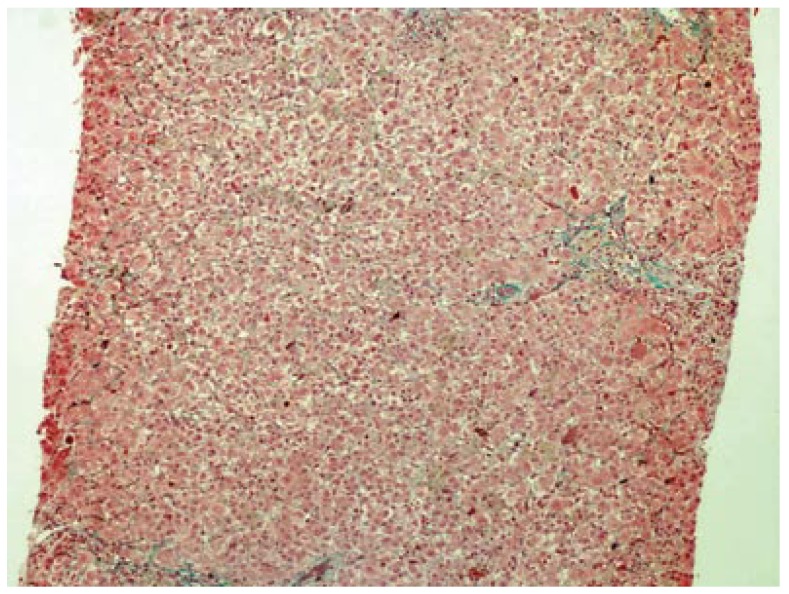
We report a case of acute hepatotoxicity in a 42-year-old woman after administration of clindamycin for a dental infection. After 6 d of treatment, she had fatigue, nausea, vomiting, anorexia, pruritus and jaundice. Her laboratory analysis showed alanine aminotransferase (ALT), 1795 IU/L (normal range 0-40); aspartate aminotransferase (AST), 1337 IU/L (normal range 5-34); alkaline phosphatase (ALP), 339 IU/L (normal range 40-150); gamma-glutamyl transpeptidase (GGT), 148 IU/L (normal range 9-64 IU/L); total bilirubin, 4.1 mg/dL; direct bilirubin, 2.9 mg/dL and prothrombin time (PT), 13.5 s, with international normalized ratio (INR), 1.04. She was hospitalized, with immediate drug discontinuation. Her liver biopsy specimen showed mixed-type (both hepatocellular and cholestatic) hepatic injury, compatible with a diagnosis of drug-induced hepatitis. An objective causality assessment using the Naranjo probability scale suggested that clindamycin was the probable cause of the acute hepatitis. In susceptible individuals, clindamycin use may lead to acute mixed-type liver toxicity. Complete recovery may be possible if the drug is discontinued before severe liver injury is established.
Figures
References
-
- Mazur D, Schug BS, Evers G, Larsimont V, Fieger-Büschges H, Gimbel W, Keilbach-Bermann A, Blume HH. Bioavailability and selected pharmacokinetic parameters of clindamycin hydrochloride after administration of a new 600 mg tablet formulation. Int J Clin Pharmacol Ther. 1999;37:386–392. - PubMed
-
- DeHaan RM, Metzler CM, Schellenberg D, VandenBosch WD, Masson EL. Pharmacokinetic studies of clindamycin hydrochloride in humans. Int J Clin Pharmacol. 1972;6:105–119. - PubMed
-
- Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, Janecek E, Domecq C, Greenblatt DJ. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–245. - PubMed
-
- Lee WM. Drug-induced hepatotoxicity. N Engl J Med. 2003;349:474–485. - PubMed
-
- Farrel GC. Liver disease caused by drugs, anesthetics and toxins. In: Mark Feldman, Lawrence S Friedman, Marvin H., editors. Sleisenger and Fordtran's gastrointestinal and liver disease: pathophysiology, diagnosis, management. 7th ed. Philadelphia: Saunders; 2002. pp. 1403–1437.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
