

Vagal paragangliomas: two case reports
- PMID: 17883192
- PMCID: PMC2640040
Vagal paragangliomas: two case reports
Abstract
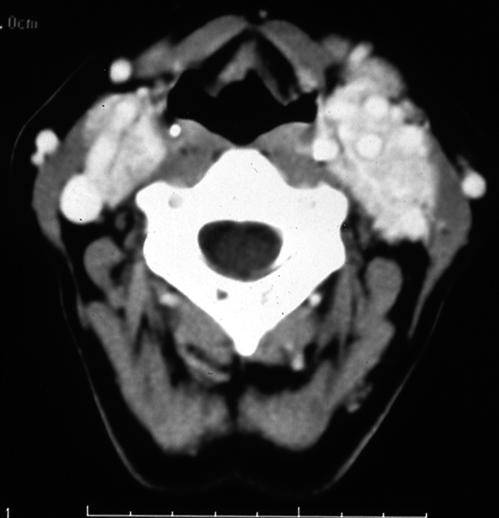
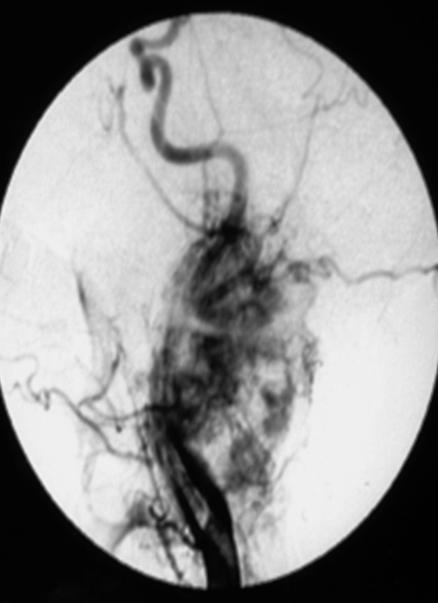
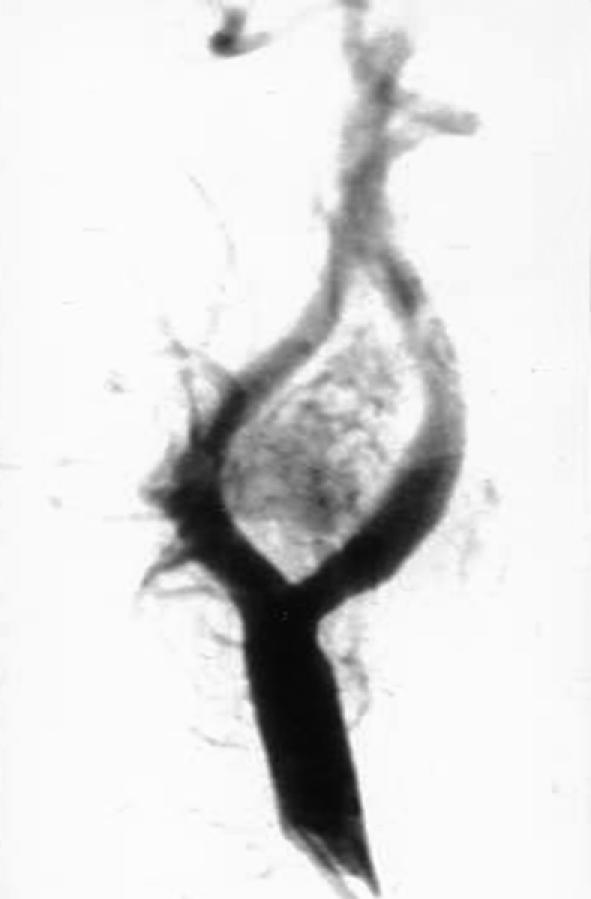
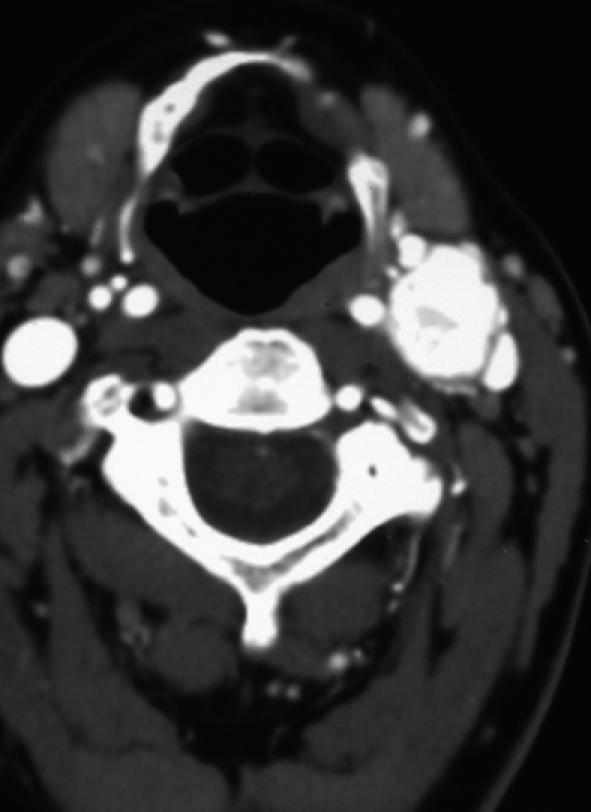
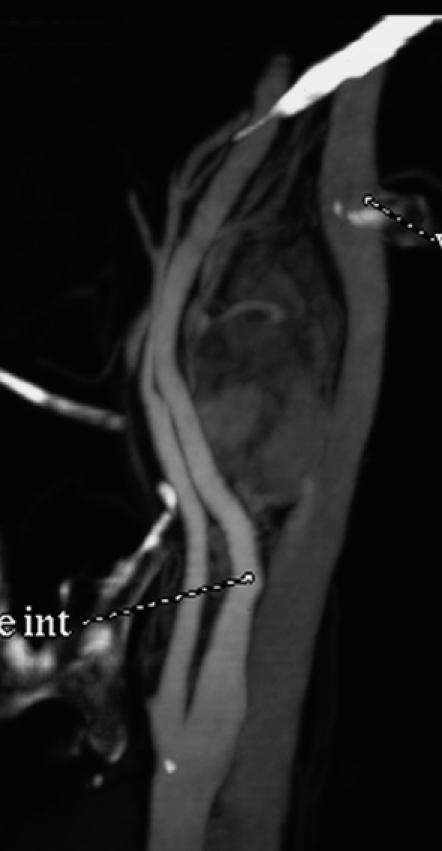
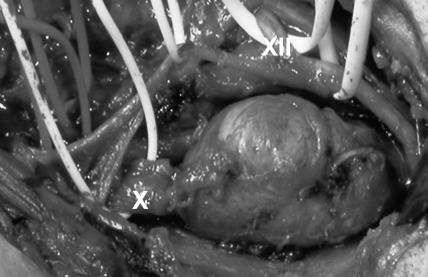
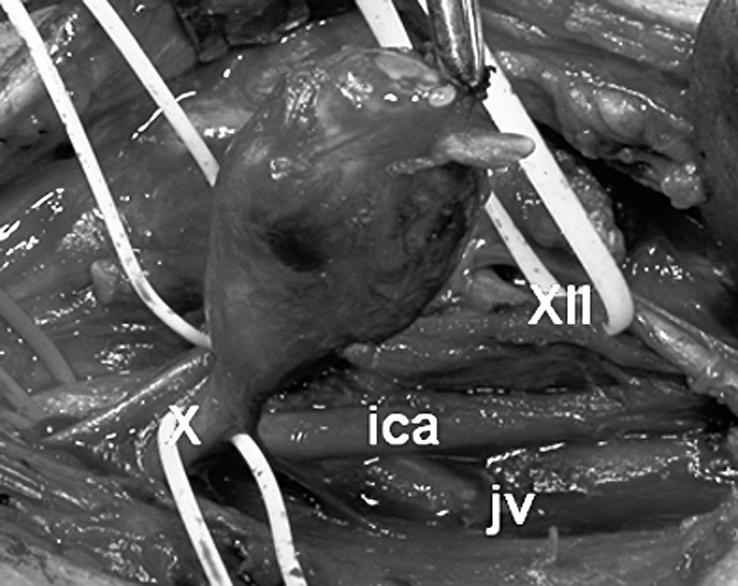
Two uncommon cases of paragangliomas arising from the vagus nerve are described. The first patient underwent surgery for suspected carotid body tumour. In the second patient, computed tomography scan and digital angiography allowed a correct pre-operative diagnosis to be made. These cases confirm the prevalence of vagal paragangliomas in female sex and middle age, and the possibility of multiple similar tumours in the same patient. Histological benign features, absence of neurological symptoms, of local invasion or intracranial extension confirm the frequent benign behaviour of these neoplasms. Lack of catecholamine secretion confirms the low incidence of functioning tumours. Contrast computed tomography and digital angiography still remain the gold standard reliable instruments for diagnosis despite the success of magnetic resonance imaging, magnetic resonance angiography and octreotide scintigraphy to detect head and neck paragangliomas. A transcervical approach, without mandibulotomy, is suitable too for large tumours but complete removal, with sparing of involved segments of the vagus nerve, is rarely possible. Post-operative neurological morbidity is still an unsolved issue and, therefore, rehabilitation of deglutition and phonation is an integral part of management.
In questo articolo riportiamo due rari casi di paraganglioma vagale. La prima paziente è stata operata con il sospetto di tumore del glomo carotideo mentre, nel secondo caso, l’angio TC e l’angiografia digitale hanno consentito una corretta diagnosi pre-operatoria. L’istologia favorevole, l’assenza di sintomi neurologici, la mancanza di invasività locale e di estensione intracranica hanno caratterizzato l’andamento benigno dei tumori. L’assenza di catecolamine e derivati nel sangue e nelle urine ha confermato la bassa incidenza di forme secernenti. Queste osservazioni confermano la predilezione del paraganglioma vagale per il sesso femminile e l’età media, e la possibilità di paragangliomi multipli nello stesso paziente. Angio TC ed angiografia digitale risultano indagini diagnostiche ancora valide nonostante i successi di RM, angio RM e scintigrafia con Octreotide. L’approccio cervicale senza mandibulotomia risulta adeguato alla rimozione di tumori anche di grandi dimensioni, mentre l’asportazione completa della lesione con conservazione del tratto di vago interessato è raramente possibile. Il problema della morbilità neurologica post-operatoria è ancora irrisolto così che la riabilitazione dei meccanismi di deglutizione e fonazione costituisce parte integrante del trattamento.
Figures


References
-
- Netterville JL, Jackson CG, Miller FR, Wanamaker JR, Glasscock ME. Vagal paraganglioma: a review of 46 patients treated during a 20-year period. Arch Otolaryngol Head Neck Surg 1998;124:1133-40. - PubMed
-
- Groblewski JC, Thekdi A, Carrau RL. Secreting vagal paraganglioma. Am J Otolaryngol 2004;25:295-300. - PubMed
-
- Urquhart AC, Johnson JT, Myers EN, Schecther GL. Glomus vagale: paraganglioma of the vagus nerve. Laryngoscope 1994;104:440-5. - PubMed
-
- Myers EN, Johnson JT, Curtin HD. Tumours of the parapharyngeal space. In: Myers EN, Suen JY, editors. Cancer of the head and neck. 3rd edn. Philadelphia, PA: Saunders; 1966. p. 562-85.
-
- Endicott JN, Maniglia AJ. Glomus vagale. Laryngoscope 1980;90:1604-11. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources