

Enhanced transmural fiber rotation and connexin 43 heterogeneity are associated with an increased upper limit of vulnerability in a transgenic rabbit model of human hypertrophic cardiomyopathy
- PMID: 17885214
- PMCID: PMC2366809
- DOI: 10.1161/CIRCRESAHA.107.161240
Enhanced transmural fiber rotation and connexin 43 heterogeneity are associated with an increased upper limit of vulnerability in a transgenic rabbit model of human hypertrophic cardiomyopathy
Abstract
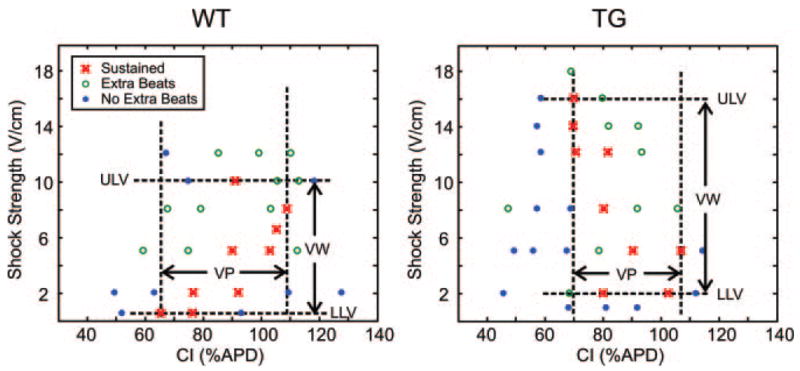
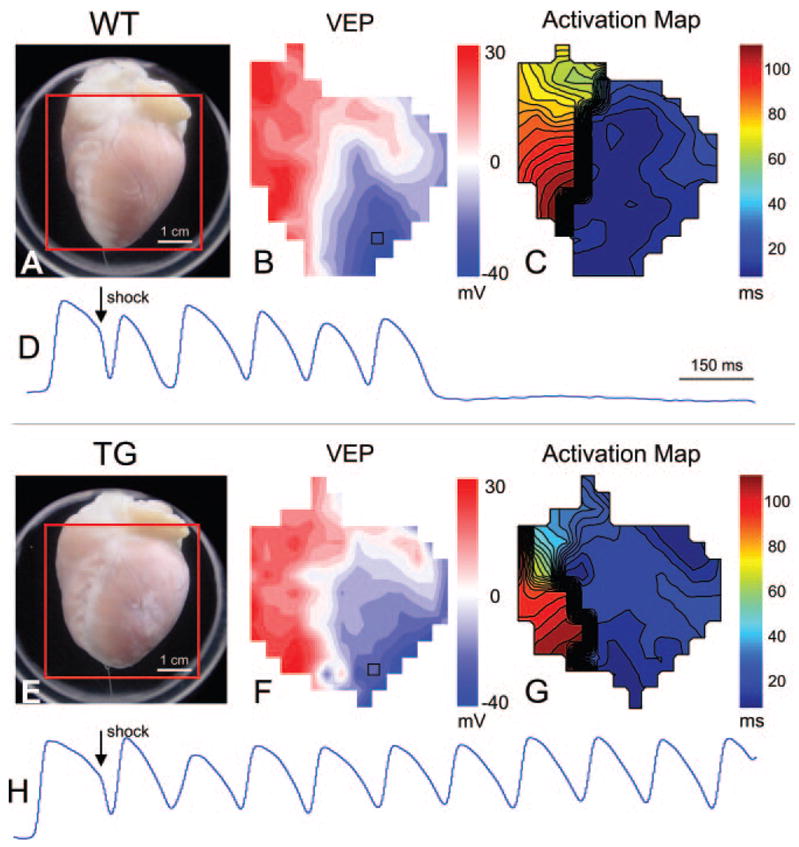
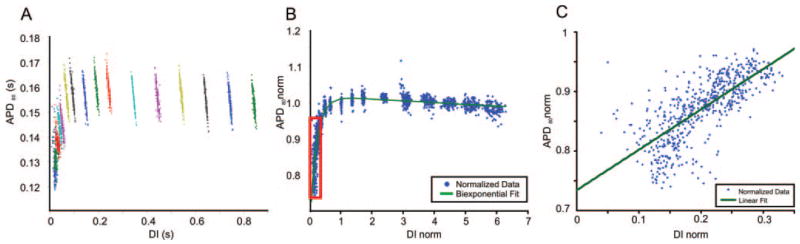
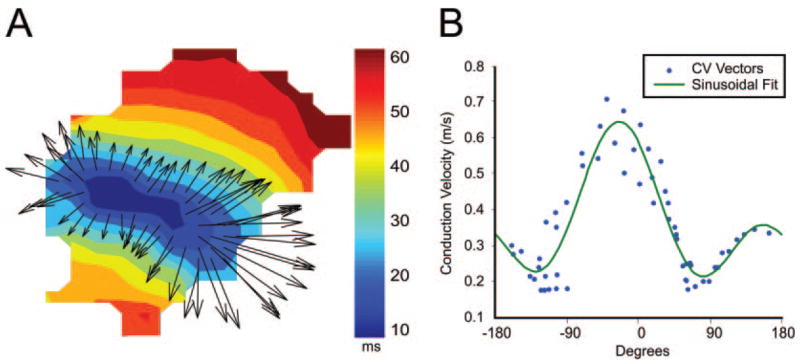
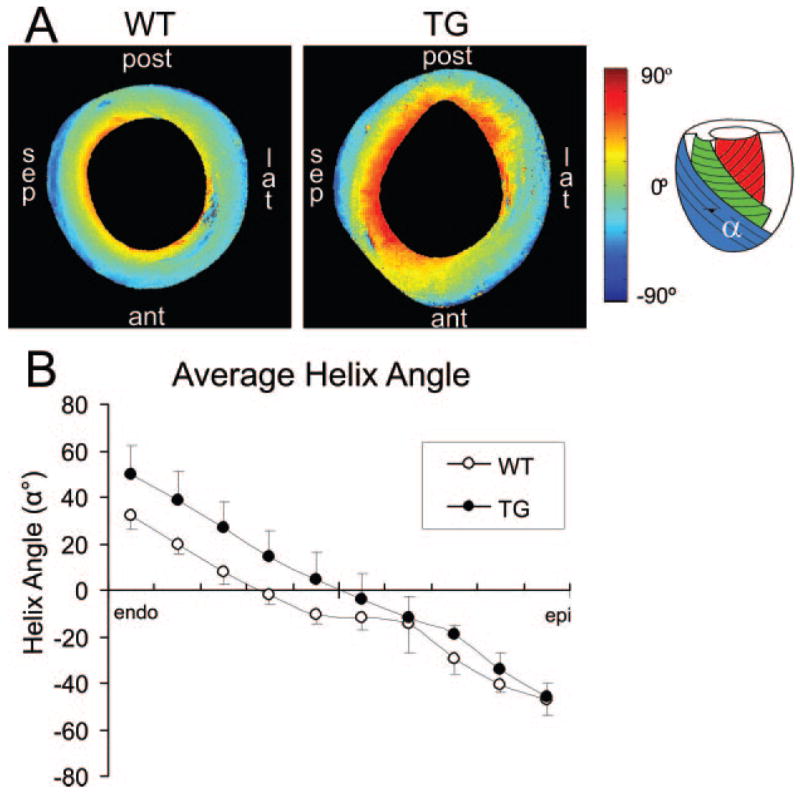
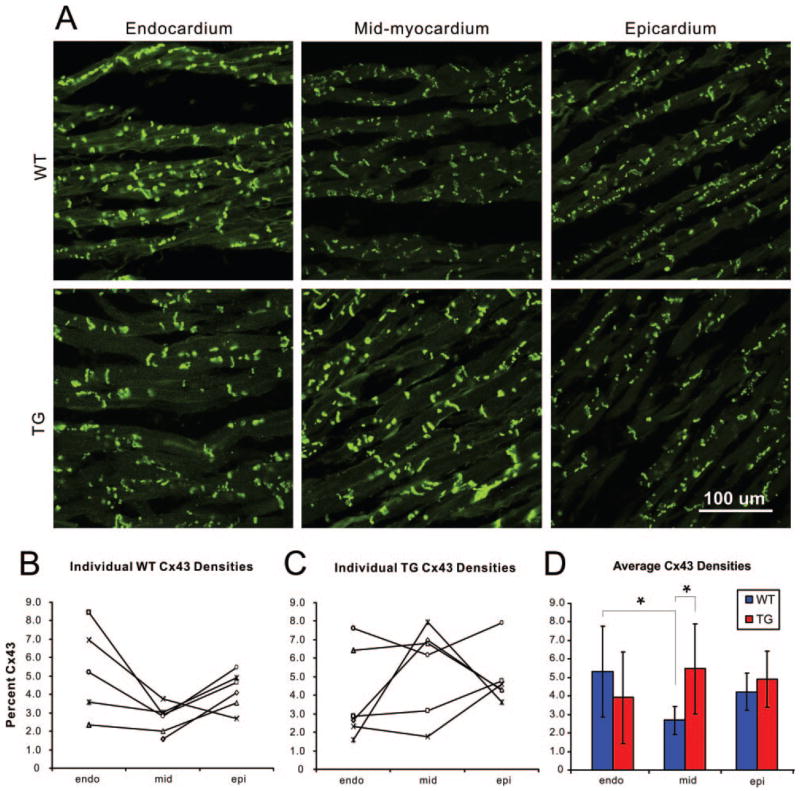
Human hypertrophic cardiomyopathy, characterized by cardiac hypertrophy and myocyte disarray, is the most common cause of sudden cardiac death in the young. Hypertrophic cardiomyopathy is often caused by mutations in sarcomeric genes. We sought to determine arrhythmia propensity and underlying mechanisms contributing to arrhythmia in a transgenic (TG) rabbit model (beta-myosin heavy chain-Q403) of human hypertrophic cardiomyopathy. Langendorff-perfused hearts from TG (n=6) and wild-type (WT) rabbits (n=6) were optically mapped. The upper and lower limits of vulnerability, action potential duration (APD) restitution, and conduction velocity were measured. The transmural fiber angle shift was determined using diffusion tensor MRI. The transmural distribution of connexin 43 was quantified with immunohistochemistry. The upper limit of vulnerability was significantly increased in TG versus WT hearts (13.3+/-2.1 versus 7.4+/-2.3 V/cm; P=3.2e(-5)), whereas the lower limits of vulnerability were similar. APD restitution, conduction velocities, and anisotropy were also similar. Left ventricular transmural fiber rotation was significantly higher in TG versus WT hearts (95.6+/-10.9 degrees versus 79.2+/-7.8 degrees; P=0.039). The connexin 43 density was significantly increased in the mid-myocardium of TG hearts compared with WT (5.46+/-2.44% versus 2.68+/-0.77%; P=0.024), and similar densities were observed in the endo- and epicardium. Because a nearly 2-fold increase in upper limit of vulnerability was observed in the TG hearts without significant changes in APD restitution, conduction velocity, or the anisotropy ratio, we conclude that structural remodeling may underlie the elevated upper limit of vulnerability in human hypertrophic cardiomyopathy.
Figures
References
-
- Maron BJ, Shirani J, Poliac LC, Mathenge R, Roberts WC, Mueller FO. Sudden death in young competitive athletes. Clinical, demographic, and pathological profiles. JAMA. 1996;276:199–204. - PubMed
-
- Maron BJ, Shen WK, Link MS, Epstein AE, Almquist AK, Daubert JP, Bardy GH, Favale S, Rea RF, Boriani G, Estes NA, III, Spirito P. Efficacy of implantable cardioverter-defibrillators for the prevention of sudden death in patients with hypertrophic cardiomyopathy. N Engl J Med. 2000;342:365–373. - PubMed
-
- Maron BJ, Estes NA, III, Maron MS, Almquist AK, Link MS, Udelson JE. Primary prevention of sudden death as a novel treatment strategy in hypertrophic cardiomyopathy. Circulation. 2003;107:2872–2875. - PubMed
-
- Davies MJ, McKenna WJ. Hypertrophic cardiomyopathy-pathology and pathogenesis. Histopathology. 1995;26:493–500. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
