

CT and MR characteristics of cerebral sparganosis
- PMID: 17885230
- PMCID: PMC8134205
- DOI: 10.3174/ajnr.A0659
CT and MR characteristics of cerebral sparganosis
Abstract
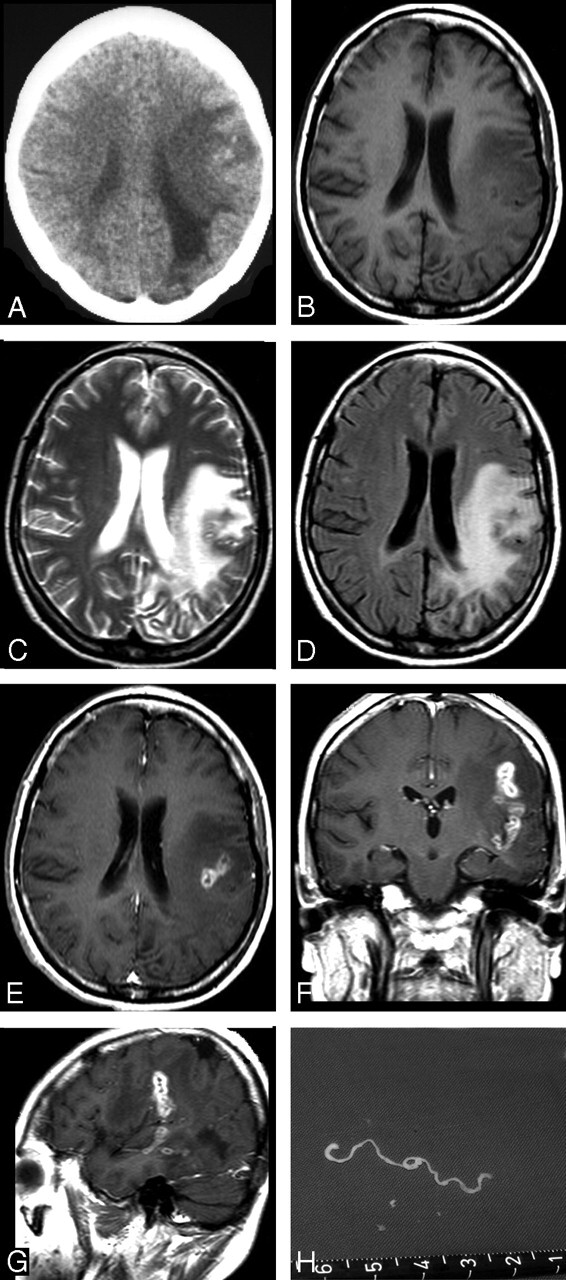
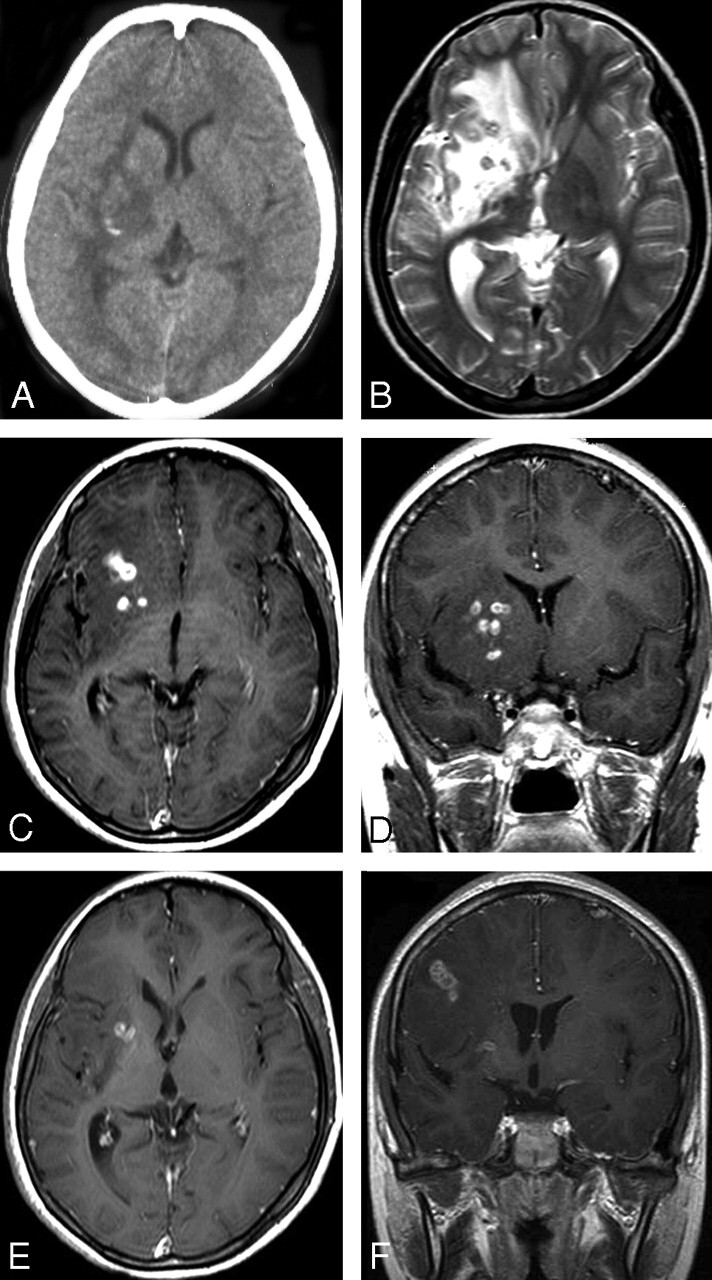
Background and purpose: Sparganosis is a rare parasitic infection in humans by a larval cestode of the genus Spirometra. Preoperative diagnosis of cerebral sparganosis in the past has been very difficult. Our objective was to evaluate the CT and MR features of cerebral sparganosis in order to make a definite diagnosis.
Materials and methods: We retrospectively reviewed 25 patients (13 male and 12 female; age range, 9-83 years) who proved to have cerebral sparganosis. Fifteen patients underwent MR imaging: 2 patients had CT scanning, and the remaining 8 had both CT and MR scanning. We focused on evaluating the imaging features on CT and MR.
Results: All patients showed edema and degeneration of cerebral white matter. All but 1 had a unilateral lesion. Twenty-two patients had ipsilateral ventricular dilation. The new finding was a tunnel sign, approximately 4 cm in length and 0.8 cm in width, column or fusiform shaped on postcontrast coronal and sagittal MR images (n = 10). Thirteen patients showed bead-like enhancement, but solitary ring enhancement was common on the CT images (n = 2). The wall of the ring and tunnel appeared isointense or slightly hyperintense on T2-weighted images. Punctate calcifications were seen in 6 patients on CT images but only in 3 patients on the MR images. Hemorrhage was seen in 4 patients on the MR images. An intact whitish, stringlike, living worm was found (n = 5).
Conclusion: The most characteristic finding was a tunnel sign on postcontrast MR images. The most common finding was bead-shaped enhancement. MR is superior to CT in demonstrating the extent and number of lesions, except punctate calcifications. Combined with clinical data and enzyme-linked immunosorbent assay, the preoperative diagnosis of cerebral sparganosis could be established on MR imaging.
Figures

References
-
- Mueller JF. The biology of Spirometra. J Parasitol 1974;60:3–14 - PubMed
-
- Muller JF, Hart EP, Walsh WP. Human sparganosis in the United States. J Parasitol 1963;49:294–96
-
- Dunn IJ, Palmer PE. Sparganosis. Semin Roentgenol 1998;33:86–88 - PubMed
-
- Chang KH, Cho SY, Chi JG, et al. Cerebral sparganosis: CT characteristics. Radiology 1987;165:505–10 - PubMed
-
- Fan KJ, Pezeshkpour GH. Cerebral sparganosis. Neurology 1986;36:1249–51 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous