

Long-term follow-up of cerebral aneurysms after endovascular therapy prediction and outcome of retreatment
- PMID: 17885238
- PMCID: PMC8134224
- DOI: 10.3174/ajnr.A0649
Long-term follow-up of cerebral aneurysms after endovascular therapy prediction and outcome of retreatment
Abstract
Background and purpose: The purpose of this study was to analyze angiographic and clinical results before and after additional endovascular therapy in patients with previously coiled but reopened cerebral aneurysms and to identify possible risk factors for retreatment of an aneurysm.
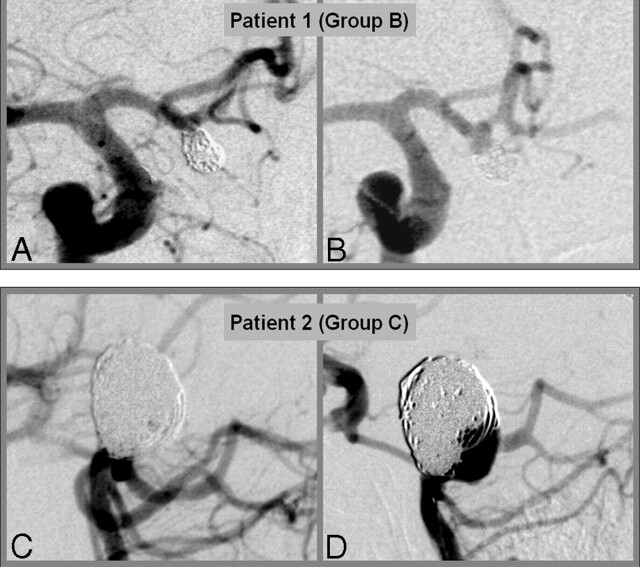
Materials and methods: Follow-up with selective digital subtraction angiography was performed in 323/596 (54.2%) patients harboring 342 aneurysms with a mean follow-up time of 28.6 months. The patients were divided into 3 groups: group A, who remained stable after initial treatment; group B, who showed minor morphologic changes; and group C, who underwent repeat treatment. Univariate and multivariate regression analyses were performed to determine possible risk factors for aneurysmal retreatment.
Results: Single or multiple retreatment was performed in 33 of 323 (10.2%) patients. Retreatment of small aneurysms (< or =10 mm) with small necks (< or =4 mm) was performed in 6 of 214 aneurysms. When summarizing all other aneurysms as a "risk group" (n = 128), the odds ratio (OR) for retreatment in the "risk group" was 3.11 (95% CI: 1.43-6.75; P = .004). In patients with residual aneurysm after the first treatment, OR for retreatment was 3.96 (95% CI: 1.48-10.65; P = .006), whereas a neck remnant, clinical presentation, and aneurysmal localization were not predictive. We observed no resulting morbidity and mortality from the 33 retreatment procedures.
Conclusion: In our series, the retreatment of aneurysmal recurrences was a safe procedure. The best single predictors of aneurysmal recurrence were aneurysmal anatomy (neck width >4 mm and diameter >10 mm) and the presence of a residual aneurysm after initial treatment. A limitation in our study was the significant number of patients lost to follow-up (22.7%).
Figures
References
-
- Henkes H, Fischer S, Weber W, et al. Endovascular coil occlusion of 1811 intracranial aneurysms: early angiographic and clinical results. Neurosurgery 2004;54:268–80; discussion 280–85 - PubMed
-
- Molyneux A, Kerr R, Stratton I, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360:1267–74 - PubMed
-
- Molyneux A, Kerr RS, Yu LM, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet 2005;366:809–17 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical