

Diagnostic value of high-resolution MR imaging in giant cell arteritis
- PMID: 17885247
- PMCID: PMC8134183
- DOI: 10.3174/ajnr.A0638
Diagnostic value of high-resolution MR imaging in giant cell arteritis
Abstract
Background and purpose: Clinical indications of giant cell arteritis may be unspecific, and noninvasive diagnosis is often difficult. This study investigated the hypothesis that high-resolution MR imaging of the superficial cranial arteries is a noninvasive imaging technique that can detect the occurrence of giant cell arteritis.
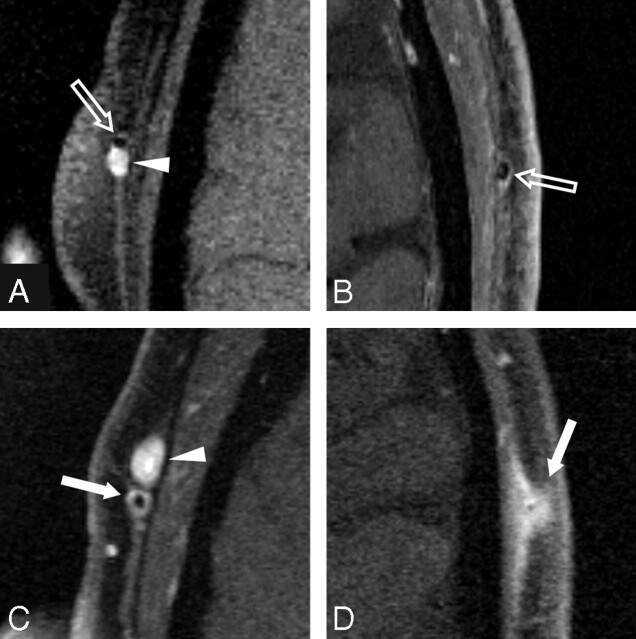
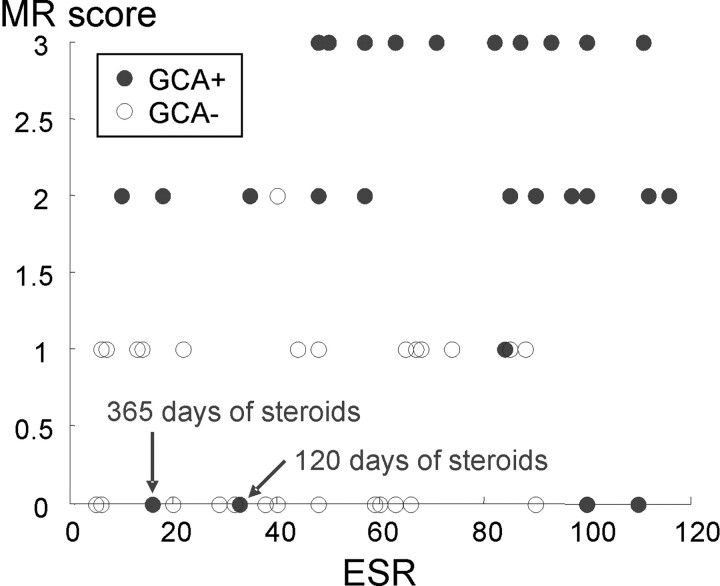
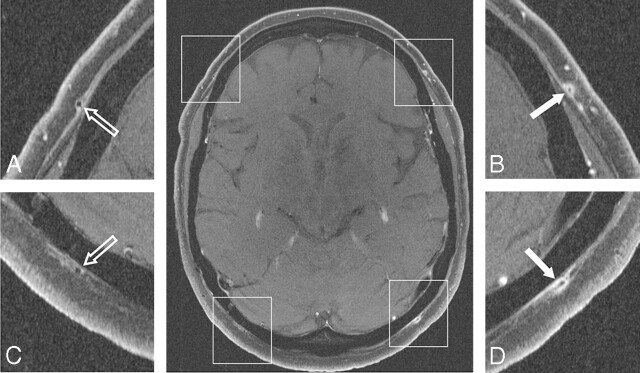
Materials and methods: Contrast-enhanced, high-resolution MR imaging was performed on 64 consecutive patients with suspected giant cell arteritis. Mural thickness, lumen diameter, and a mural contrast enhancement score were assessed with T1-weighted spin-echo images with submillimeter in-plane spatial resolution. The final rheumatologist's diagnosis according to the clinical criteria of the American College of Rheumatology including laboratory tests and results of temporal artery biopsies from 32 patients was used as a "gold standard" for the evaluation of the MR imaging findings.
Results: All of the examinations provided diagnostic image quality. Evaluation of the mural inflammatory MR imaging signs for diagnosing vasculitis resulted in a sensitivity of 80.6% and a specificity of 97.0%. In comparison, histology results alone showed a sensitivity of 77.8% and specificity of 100%. The mean wall thickness increased significantly from 0.39 mm (+/-0.18 mm) to 0.74 mm (+/-0.32 mm; P < .001), and the lumen diameter decreased significantly from 0.84 mm (+/-0.29 mm) to 0.65 mm (+/-0.38 mm; P < .05) for patients with giant cell arteritis.
Conclusion: Contrast-enhanced, high-resolution MR imaging allows noninvasive assessment of mural inflammation in giant cell arteritis with good diagnostic certainty. Measures of mural thickening and contrast enhancement can be obtained in these small vessels and provide valuable vasculitic MR imaging findings.
Figures
References
-
- Horton B, Magath T, Brown G. An undescribed form of arteritis of the temporal vessels. Proc Mayo Clin 1932;7:700–01
-
- Salvarani C, Cantini F, Boiardi L, et al. Polymyalgia rheumatica and giant-cell arteritis. N Engl J Med 2002;347:261–71 - PubMed
-
- Bley TA, Weiben O, Uhl M, et al. Assessment of the cranial involvement pattern of giant cell arteritis with 3T magnetic resonance imaging. Arthritis Rheum 2005;52:2470–77 - PubMed
-
- Nuenninghoff DM, Hunder GG, Christianson TJ, et al. Incidence and predictors of large-artery complication (aortic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: a population-based study over 50 years. Arthritis Rheum 2003;48:3522–31 - PubMed
-
- Pfadenhauer K, Weber H. Giant cell arteritis of the occipital arteries–a prospective color coded duplex sonography study in 78 patients. J Neurol 2003;250:844–49 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical