

Treatment of carotid cavernous fistulas using covered stents: midterm results in seven patients
- PMID: 17885249
- PMCID: PMC8134221
- DOI: 10.3174/ajnr.A0636
Treatment of carotid cavernous fistulas using covered stents: midterm results in seven patients
Abstract
Background and purpose: Carotid cavernous fistulas (CCF) can be effectively treated by using different therapeutic alternatives such as detachable balloons and detachable coils, alone or in combination with N-butyl-2-cyanoacrylate (n-BCA) or Onyx. Stents have also been used in an attempt to improve preservation of the parent artery while still occluding the fistula. We present our experience using balloon-expandable covered stents to treat CCF, focusing on arterial wall reconstruction. To our knowledge, this is the first series with midterm follow-up between 3 months and 3.5 years.
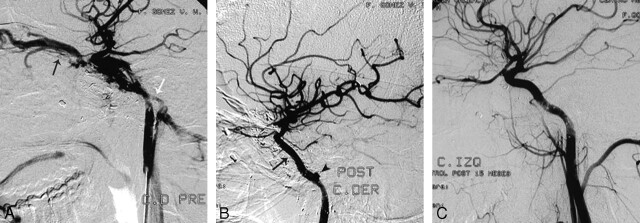
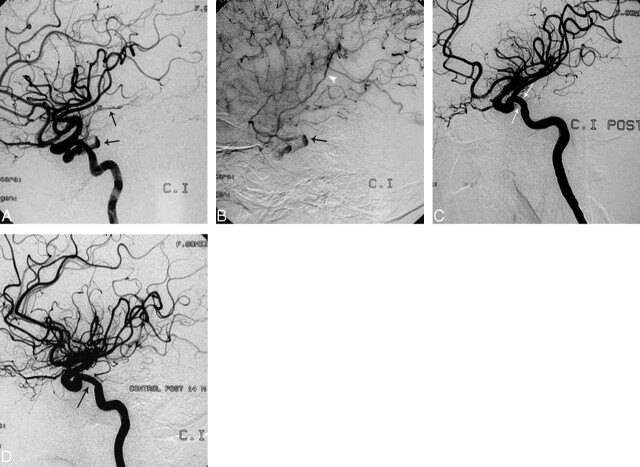
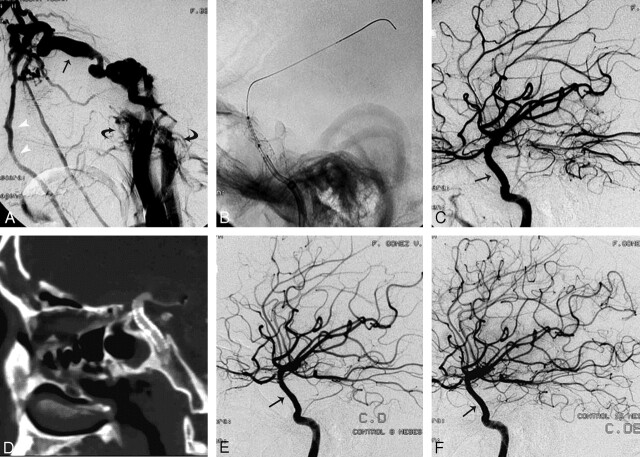
Materials and methods: From the 46 CCF treated at our institution between November 1998 and September 2006, a total of 7 posttraumatic direct CCF were treated using polytetrafluoroethylene (PTFE)-covered stents between April 2003 and September 2006. Five were treated with covered stents alone. One patient with transection of the internal carotid artery (ICA) first underwent bare stent placement to provide support for the covered stent. One patient had to be treated with coils and n-BCA.
Results: Control angiograms obtained in the 7 patients demonstrated occlusion of the fistula and preservation of the ICA in all cases. There was no mortality and no immediate postprocedural morbidity. There was 1 case of morbidity identified at 1-month follow-up with asymptomatic occlusion of the ICA; the other 6 patients had angiographic follow-up between 3 and 42 months (mean, 18.4 months), with persistent occlusion of the fistulas, patent stent grafts, and no significant intimal hyperplasia.
Conclusions: PTFE-covered stents are evolving as a promising intracranial therapeutic alternative to treat CCF and preserve the parent artery by reconstructing the arterial wall. They should be considered in patients in whom fistulas cannot be successfully occluded with detachable balloons or detachable coils. More investigation is required to further develop their specifications and indications.
Figures
Similar articles
-
Carotid cavernous fistulas treated by endovascular covered stent grafts with follow-up results.Br J Neurosurg. 2010 Aug;24(4):435-40. doi: 10.3109/02688697.2010.487127. Br J Neurosurg. 2010. PMID: 20515263 Review.
-
[Diagnosis and treatment of carotid-cavernous fistula: analysis of 28 patients].Zhonghua Yi Xue Za Zhi. 2012 Jun 5;92(21):1458-62. Zhonghua Yi Xue Za Zhi. 2012. PMID: 22944030 Chinese.
-
Endovascular treatment of post-traumatic direct carotid-cavernous fistulas: A single-center experience.J Clin Neurosci. 2011 Jan;18(1):24-8. doi: 10.1016/j.jocn.2010.06.008. J Clin Neurosci. 2011. PMID: 20888773
-
Placement of covered stents for the treatment of direct carotid cavernous fistulas.AJNR Am J Neuroradiol. 2009 Aug;30(7):1342-6. doi: 10.3174/ajnr.A1583. Epub 2009 Apr 2. AJNR Am J Neuroradiol. 2009. PMID: 19342540 Free PMC article. Clinical Trial.
-
Endovascular techniques for treatment of carotid-cavernous fistula.J Neuroophthalmol. 2009 Mar;29(1):62-71. doi: 10.1097/WNO.0b013e3181989fc0. J Neuroophthalmol. 2009. PMID: 19458580 Review.
Cited by
-
Transarterial Embolization of Direct Carotid Cavernous Fistulas with the Double-balloon Technique.Interv Neuroradiol. 2008 Nov 11;14 Suppl 2(Suppl 2):13-7. doi: 10.1177/15910199080140S204. Epub 2009 Jan 2. Interv Neuroradiol. 2008. PMID: 20557795 Free PMC article.
-
Balloon-assisted coiling of the cavernous sinus to treat direct carotid cavernous fistula. A single center experience of 13 consecutive patients.Interv Neuroradiol. 2013 Sep;19(3):344-52. doi: 10.1177/159101991301900312. Epub 2013 Sep 26. Interv Neuroradiol. 2013. PMID: 24070084 Free PMC article. Clinical Trial.
-
Multiple unilateral traumatic carotid-cavernous sphenoid sinus fistulas with associated massive epistaxis: a consequence of parkour.Ochsner J. 2015 Spring;15(1):92-6. Ochsner J. 2015. PMID: 25829888 Free PMC article.
-
Endovascular treatment of carotid cavernous sinus fistula: A systematic review.World J Radiol. 2013 Apr 28;5(4):143-55. doi: 10.4329/wjr.v5.i4.143. World J Radiol. 2013. PMID: 23671750 Free PMC article.
-
Endovascular graft-stent placement for treatment of traumatic carotid cavernous fistulas.J Korean Neurosurg Soc. 2009 Dec;46(6):572-6. doi: 10.3340/jkns.2009.46.6.572. Epub 2009 Dec 31. J Korean Neurosurg Soc. 2009. PMID: 20062575 Free PMC article.
References
-
- Serbinenko FA. Balloon catheterization and occlusion of major cerebral vessels. J Neurosurg 1974;41:125–45 - PubMed
-
- Debrun G, Lacour P, Caron JP, et al. Experimental approach to the treatment of carotid-cavernous fistulas with an inflatable and isolated balloon. Neuroradiology 1975;9:9–12
-
- Debrun G, Lacour P, Caron JP, et al. Detachable balloon and calibrated-leak balloon techniques in the treatment of cerebral vascular lesions. J Neurosurg 1978;49:635–49 - PubMed
-
- Debrun G, Lacour P, Vinuela F, et al. Treatment of 54 traumatic carotid-cavernous fistulas. J Neurosurg 1981;55:678–92 - PubMed
-
- Lewis AI, Tomsick TA, Tew JM, et al. Long-term results in direct carotid-cavernous fistula treatment with detachable balloons. J Neurosurg 1996;84:400–04 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous