

Angiotensin-converting enzyme gene polymorphism predicts the time-course of blood pressure response to angiotensin converting enzyme inhibition in the AASK trial
- PMID: 17885551
- PMCID: PMC2792638
- DOI: 10.1097/HJH.0b013e3282b9720e
Angiotensin-converting enzyme gene polymorphism predicts the time-course of blood pressure response to angiotensin converting enzyme inhibition in the AASK trial
Abstract
Objective: It has yet to be determined whether genotyping at the angiotensin-converting enzyme (ACE) locus is predictive of blood pressure response to an ACE inhibitor.
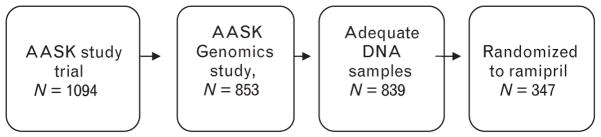
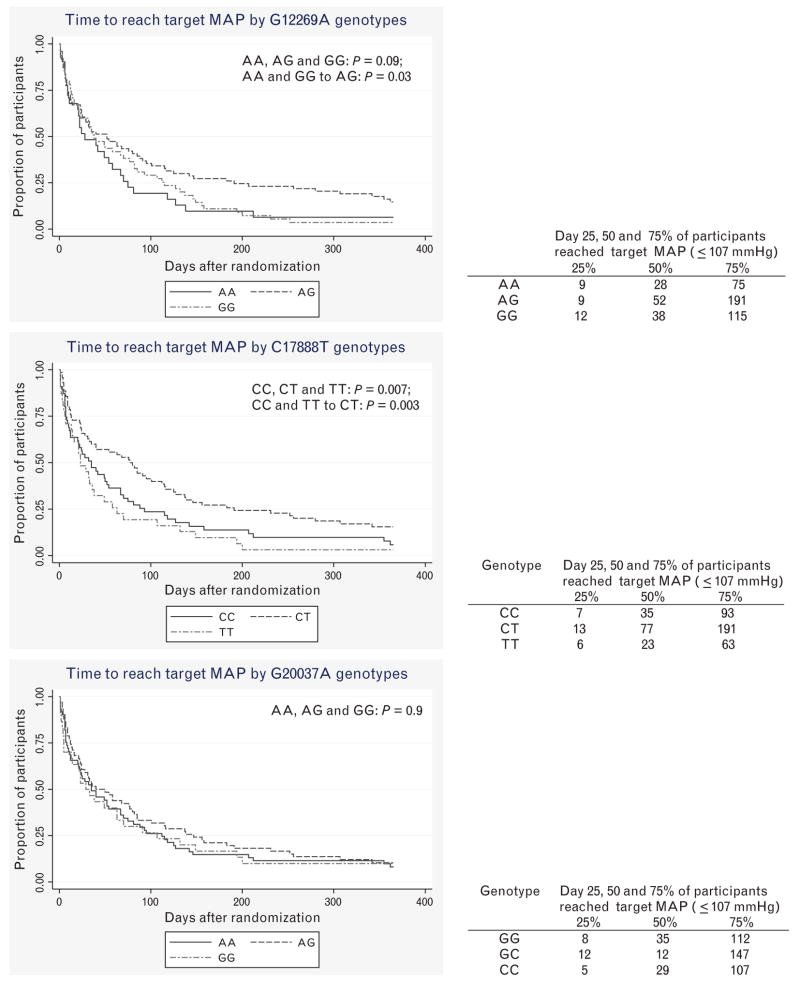
Methods: Participants from the African American Study of Kidney Disease and Hypertension trial randomized to the ACE inhibitor ramipril (n = 347) were genotyped at three polymorphisms on ACE, just downstream from the ACE insertion/deletion polymorphism (Ins/Del): G12269A, C17888T, and G20037A. Time to reach target mean arterial pressure (</=107 mmHg) was analyzed by genotype and ACE haplotype using Kaplan-Meier survival curves and Cox proportional hazard models.
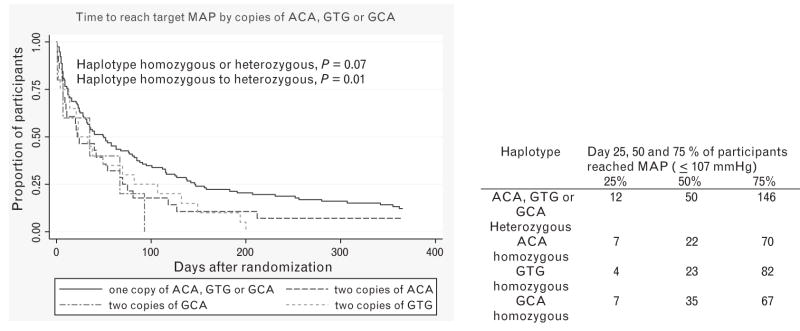
Results: Individuals with a homozygous genotype at G12269A responded significantly faster than those with a heterozygous genotype; the adjusted (average number of medications and baseline mean arterial pressure) hazard ratio (homozygous compared to heterozygous genotype) was 1.86 (95% confidence limits 1.32-3.23; P < 0.001 for G12269A genotype). The adjusted hazard ratio for participants with homozygous ACE haplotypes compared to those heterozygous ACE haplotypes was 1.40 (1.13-1.75; P = 0.003 for haplotype). The ACE genotype effects were specific for ACE inhibition (i.e., not seen among those randomized to a calcium channel blocker), and were independent of population stratification.
Conclusions: African-Americans with a homozygous genotype at G12269A or homozygous ACE haplotypes responded to ramipril significantly faster than those with a heterozygous genotype or heterozygous haplotypes, suggesting that heterosis may be an important determinant of responsiveness to an ACE inhibitor. These associations may be a result of biological activity of this polymorphism, or of linkage disequilibrium with nearby variants such as the ACE Ins/Del, perhaps in the regulation of ACE splicing.
Conflict of interest statement
The authors do not have any conflict of interest or disclosures to report.
Figures

Similar articles
-
Relationship between polymorphism of the angiotensin-converting enzyme gene and the response to angiotensin-converting enzyme inhibition in hypertensive patients.Hypertens Res. 2003 Nov;26(11):881-6. doi: 10.1291/hypres.26.881. Hypertens Res. 2003. PMID: 14714579 Clinical Trial.
-
Impact of angiotensin-converting enzyme gene polymorphism on proteinuria and arterial hypertension.Coll Antropol. 2013 Sep;37(3):765-70. Coll Antropol. 2013. PMID: 24308214
-
Correlation of renin angiotensin system (RAS) candidate gene polymorphisms with response to Ramipril in patients with essential hypertension.J Postgrad Med. 2015 Jan-Mar;61(1):21-6. doi: 10.4103/0022-3859.147028. J Postgrad Med. 2015. PMID: 25511213 Free PMC article.
-
Cardiovascular risk in patients with mild renal insufficiency: implications for the use of ACE inhibitors.Presse Med. 2005 Oct 22;34(18):1303-8. doi: 10.1016/s0755-4982(05)84178-8. Presse Med. 2005. PMID: 16269994 Review.
-
Effects of renin-angiotensin system inhibition on end-organ protection: can we do better?Clin Ther. 2007 Sep;29(9):1803-24. doi: 10.1016/j.clinthera.2007.09.019. Clin Ther. 2007. PMID: 18035185 Review.
Cited by
-
African Americans, hypertension and the renin angiotensin system.World J Cardiol. 2014 Sep 26;6(9):878-89. doi: 10.4330/wjc.v6.i9.878. World J Cardiol. 2014. PMID: 25276290 Free PMC article. Review.
-
CYP3A4 and CYP3A5 polymorphisms and blood pressure response to amlodipine among African-American men and women with early hypertensive renal disease.Am J Nephrol. 2010;31(2):95-103. doi: 10.1159/000258688. Epub 2009 Nov 12. Am J Nephrol. 2010. PMID: 19907160 Free PMC article. Clinical Trial.
-
Hereditary determinants of human hypertension: strategies in the setting of genetic complexity.Hypertension. 2008 Jun;51(6):1456-64. doi: 10.1161/HYPERTENSIONAHA.107.090480. Epub 2008 Apr 14. Hypertension. 2008. PMID: 18413494 Free PMC article. Review. No abstract available.
-
Angiotensin I converting enzyme gene polymorphisms and risk of psychiatric disorders.BMC Psychiatry. 2022 May 23;22(1):351. doi: 10.1186/s12888-022-04007-w. BMC Psychiatry. 2022. PMID: 35606706 Free PMC article.
-
Serum potassium predicts time to blood pressure response among African Americans with hypertensive nephrosclerosis.J Hum Hypertens. 2013 Jun;27(6):393-6. doi: 10.1038/jhh.2012.47. Epub 2012 Nov 15. J Hum Hypertens. 2013. PMID: 23151750 Free PMC article. Clinical Trial.
References
-
- Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS. Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis. 2003;41:1–12. - PubMed
-
- Fox CS, Larson MG, Leip EP, Culleton B, Wilson PW, Levy D. Predictors of new-onset kidney disease in a community-based population. JAMA. 2004;291:844–850. - PubMed
-
- Rahman M, Brown CD, Coresh J, Davis BR, Eckfeldt JH, Kopyt N, et al. The prevalence of reduced glomerular filtration rate in older hypertensive patients and its association with cardiovascular disease: a report from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial. Arch Intern Med. 2004;164:969–976. - PubMed
-
- Klag MJ, Whelton PK, Randall BL, Neaton JD, Brancati FL, Ford CE, et al. Blood pressure and end-stage renal disease in men. N Engl J Med. 1996;334:13–18. - PubMed
-
- Berlowitz DR, Ash AS, Hickey EC, Friedman RH, Glickman M, Kader B, Moskowitz MA. Inadequate management of blood pressure in a hypertensive population. N Engl J Med. 1998;339:1957–1963. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- MD000220/MD/NIMHD NIH HHS/United States
- U01 HL064777/HL/NHLBI NIH HHS/United States
- P60 MD000220/MD/NIMHD NIH HHS/United States
- R01 DK57867/DK/NIDDK NIH HHS/United States
- K23 RR020822/RR/NCRR NIH HHS/United States
- M01 RR000071/RR/NCRR NIH HHS/United States
- HL58120/HL/NHLBI NIH HHS/United States
- U01 DK48689/DK/NIDDK NIH HHS/United States
- R01 DK060702/DK/NIDDK NIH HHS/United States
- P01 HL058120/HL/NHLBI NIH HHS/United States
- DK60702/DK/NIDDK NIH HHS/United States
- U01 DK048689/DK/NIDDK NIH HHS/United States
- 5U01 HL064777-07/HL/NHLBI NIH HHS/United States
- MO1-RR00071/RR/NCRR NIH HHS/United States
- R01 DK057867/DK/NIDDK NIH HHS/United States
- K23 RR020822-01A1/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
