

Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2007 update
- PMID: 17885691
- PMCID: PMC2806792
- DOI: 10.1155/2007/830570
Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease - 2007 update
Abstract
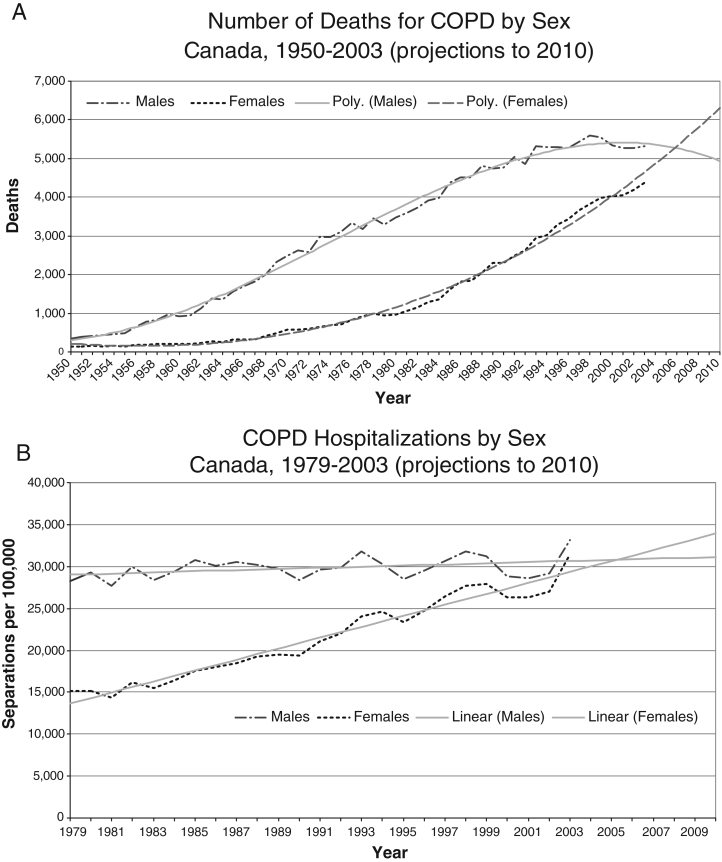
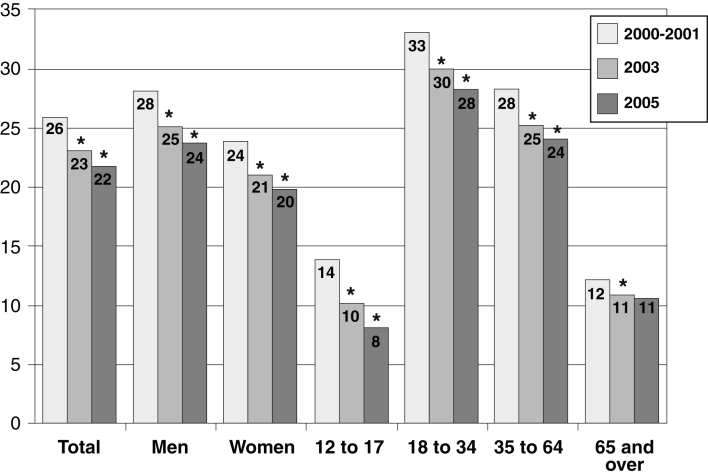
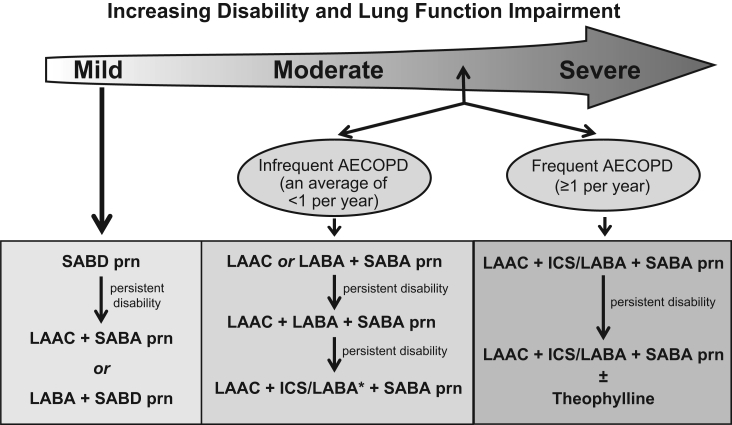
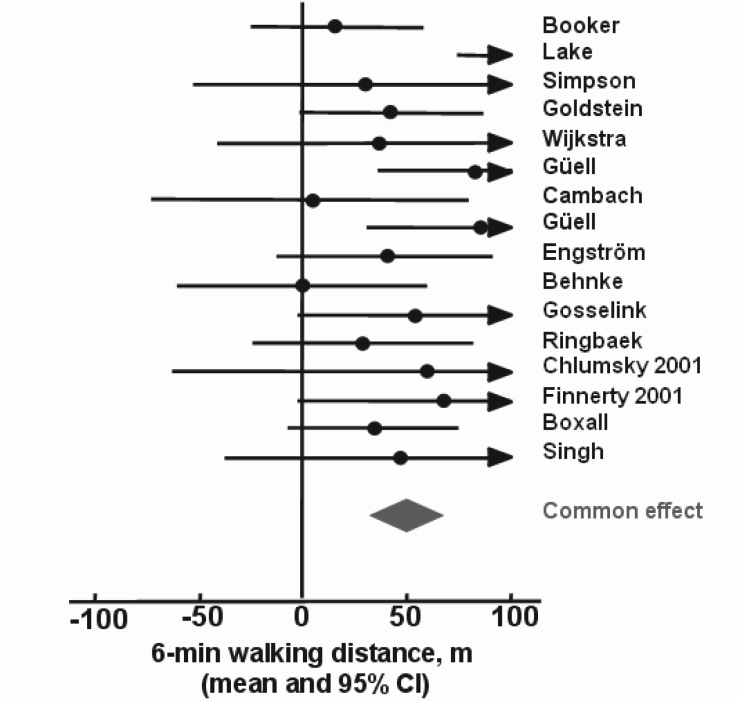
Chronic obstructive pulmonary disease (COPD) is a major respiratory illness in Canada that is both preventable and treatable. Our understanding of the pathophysiology of this complex condition continues to grow and our ability to offer effective treatment to those who suffer from it has improved considerably. The purpose of the present educational initiative of the Canadian Thoracic Society (CTS) is to provide up to date information on new developments in the field so that patients with this condition will receive optimal care that is firmly based on scientific evidence. Since the previous CTS management recommendations were published in 2003, a wealth of new scientific information has become available. The implications of this new knowledge with respect to optimal clinical care have been carefully considered by the CTS Panel and the conclusions are presented in the current document. Highlights of this update include new epidemiological information on mortality and prevalence of COPD, which charts its emergence as a major health problem for women; a new section on common comorbidities in COPD; an increased emphasis on the meaningful benefits of combined pharmacological and nonpharmacological therapies; and a new discussion on the prevention of acute exacerbations. A revised stratification system for severity of airway obstruction is proposed, together with other suggestions on how best to clinically evaluate individual patients with this complex disease. The results of the largest randomized clinical trial ever undertaken in COPD have recently been published, enabling the Panel to make evidence-based recommendations on the role of modern pharmacotherapy. The Panel hopes that these new practice guidelines, which reflect a rigorous analysis of the recent literature, will assist caregivers in the diagnosis and management of this common condition.
La maladie pulmonaire obstructive chronique (MPOC) est une maladie respiratoire majeure au Canada, à la fois évitable et traitable. Notre compréhension de la physiopathologie de cette maladie complexe continue d’évoluer, et notre capacité d ’offrir un traitement efficace aux personnes atteintes s’est améliorée considérablement. La présente initiative en matière d’éducation de la Société canadienne de thoracologie (SCT) vise à fournir de l’information à jour au sujet des progrès dans le domaine, afin que les patients atteints de cette maladie reçoivent des soins optimaux fondés sur des données probantes solides. Depuis la publication des dernières recommandations de prise en charge de la SCT en 2003, on a mis au jour une pléthore de nouvelles données scientifiques. Le groupe de travail de la SCT a évalué consciencieusement les conséquences de ces nouvelles connaissances en matière de soins cliniques optimaux, et le présent document contient les conclusions tirées de cet examen. Les faits saillants de cette mise à jour sont de nouvelles données épidémiologiques sur la mortalité et la prévalence de la MPOC, qui en révèlent l’émergence comme trouble de santé d’importance pour les femmes, une nouvelle rubrique sur les comorbidités de la MPOC, une plus grande attention accordée aux bienfaits significatifs de l’association des thérapies pharmacologiques et non pharmacologiques et un nouvel exposé sur la prévention des exacerbations aiguës. On propose un système révisé de stratification pour établir la gravité de l’obstruction des voies aériennes, de même que d’autres suggestions sur le meilleur moyen de procéder à l’évaluation clinique de chaque patient atteint de cette maladie complexe. Les résultats du plus grand essai clinique aléatoire jamais entrepris dans le domaine de la MPOC ont récemment été publiés, ce qui a permis au groupe de travail de présenter des recommandations probantes sur le rôle de la pharmacothérapie moderne. Le groupe de travail espère que ces nouvelles lignes de pratique, qui reflètent une analyse rigoureuse des publications récentes, aideront les dispensateurs de soins dans le diagnostic et la prise en charge de cette maladie courante.
Figures
References
-
- Ernst P, Fitzgerald J, Spier S. Canadian Asthma Consensus Conference: Summary of recommendations. Can Respir J. 1996;3:89–100.
-
- Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005;26:948–68. - PubMed
-
- Deaths by selected grouped causes, sex and geography – Canada<www.statcan.ca/english/freepub/84F0209XIE/2003000/t001_en.pdf> (Version current at July 18, 2007).
-
- Respiratory Disease in Canada www.phac-aspc.gc.ca/publicat/rdc-mrc01/pdf/rdc0901e.pdf (Version current at July 18, 2007).
-
- Ernst PP, Bourbeau J, Rainville B, Benayoun S, Suissa S. Underestimation of COPD as a cause of death. Eur Respir J. 2000;16(Suppl 31):13S.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
