

Patient-specific three-dimensional composite bone models for teaching and operation planning
- PMID: 17885790
- PMCID: PMC3043722
- DOI: 10.1007/s10278-007-9078-8
Patient-specific three-dimensional composite bone models for teaching and operation planning
Abstract
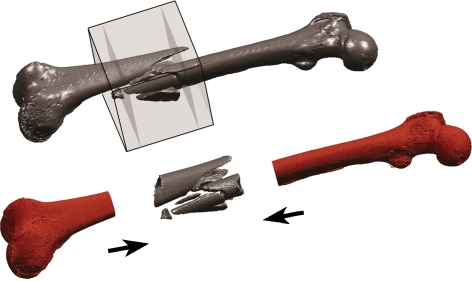
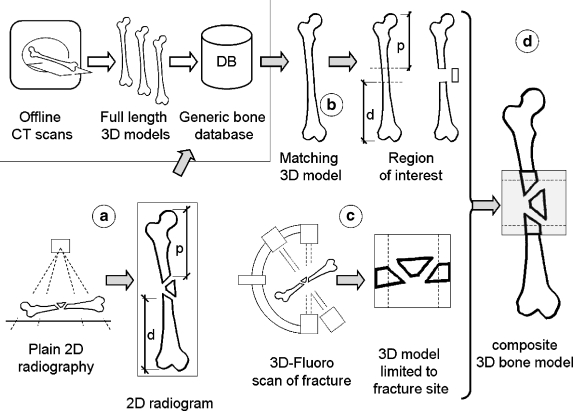
Background: Orthopedic trauma care relies on two-dimensional radiograms both before and during the operation. Understanding the three-dimensional nature of complex fractures on plain radiograms is challenging. Modern fluoroscopes can acquire three-dimensional volume datasets even during an operation, but the device limitations constrain the acquired volume to a cube of only 12-cm edge. However, viewing the surrounding intact structures is important to comprehend the fracture in its context. We suggest merging a fluoroscope's volume scan into a generic bone model to form a composite full-length 3D bone model.
Methods: Materials consisted of one cadaver bone and 20 three-dimensional surface models of human femora. Radiograms and computed tomography scans were taken before and after applying a controlled fracture to the bone. A 3D scan of the fracture was acquired using a mobile fluoroscope (Siemens Siremobil). The fracture was fitted into the generic bone models by rigid registration using a modified least-squares algorithm. Registration precision was determined and a clinical appraisal of the composite models obtained.
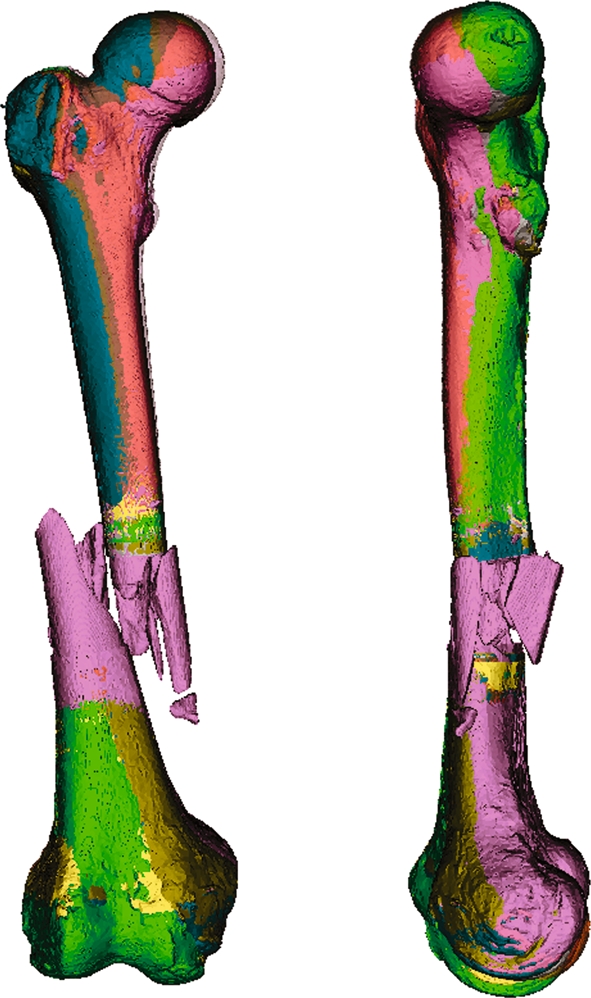
Results: Twenty composite bone models were generated. Average registration precision was 2.0 mm (range 1.6 to 2.6). Average processing time on a laptop computer was 35 s (range 20 to 55). Comparing synthesized radiograms with the actual radiograms of the fractured bone yielded clinically satisfactory results.
Conclusion: A three-dimensional full-length representation of a fractured bone can reliably be synthesized from a short scan of the patient's fracture and a generic bone model. This patient-specific model can subsequently be used for teaching, surgical operation planning, and intraoperative visualization purposes.
Figures



Similar articles
-
Comparative study of different intraoperative 3-D image intensifiers in orthopedic trauma care.J Trauma. 2009 Mar;66(3):821-30. doi: 10.1097/TA.0b013e31815edf34. J Trauma. 2009. PMID: 19276760
-
Development and validation of a generic 3D model of the distal femur.Comput Methods Biomech Biomed Engin. 2006 Oct;9(5):305-12. doi: 10.1080/10255840600935217. Comput Methods Biomech Biomed Engin. 2006. PMID: 17132616
-
Gradient-based 2-D/3-D rigid registration of fluoroscopic X-ray to CT.IEEE Trans Med Imaging. 2003 Nov;22(11):1395-406. doi: 10.1109/TMI.2003.819288. IEEE Trans Med Imaging. 2003. PMID: 14606673
-
Use of rapid prototyping and three-dimensional reconstruction modeling in the management of complex fractures.Eur J Radiol. 2011 Dec;80(3):814-20. doi: 10.1016/j.ejrad.2010.10.007. Epub 2011 Jan 22. Eur J Radiol. 2011. PMID: 21256690 Review.
-
[Intraoperative 3D imaging : Diagnostic accuracy and therapeutic benefits].Unfallchirurg. 2016 Oct;119(10):835-42. doi: 10.1007/s00113-016-0245-6. Unfallchirurg. 2016. PMID: 27646699 Review. German.
Cited by
-
Application of three-dimensional reconstruction and printing as an elective course for undergraduate medical students: an exploratory trial.Surg Radiol Anat. 2019 Oct;41(10):1193-1204. doi: 10.1007/s00276-019-02248-1. Epub 2019 Apr 27. Surg Radiol Anat. 2019. PMID: 31030233
-
Virtual Reality in Preoperative Planning of Adolescent Idiopathic Scoliosis Surgery Using Google Cardboard.Neurospine. 2021 Mar;18(1):199-205. doi: 10.14245/ns.2040574.287. Epub 2021 Mar 31. Neurospine. 2021. PMID: 33819947 Free PMC article.
-
Bone surface mapping method.PLoS One. 2012;7(3):e32926. doi: 10.1371/journal.pone.0032926. Epub 2012 Mar 8. PLoS One. 2012. PMID: 22412952 Free PMC article.
-
Computational modeling for bedside application.Heart Fail Clin. 2008 Jul;4(3):371-8. doi: 10.1016/j.hfc.2008.02.009. Heart Fail Clin. 2008. PMID: 18598988 Free PMC article.
References
-
- Rüedi TP, Buckley RE, Moran CG: AO Principles of Fracture Management, Second expanded edition (2007), Stuttgart: Thieme, 2006
-
- Messmer P, Long G, Suhm N, Hehli M, Wirth J, Regazzoni P, Jacob AL. Three-dimensional fracture simulation for preoperative planning and education. Eur J Trauma. 2001;27:171–177.
-
- Wirth S, Euler E, Linsenmaier U, Heining SM, Kotsianos D, Pfeifer KJ, Mutschler W, Reiser M. C-arm-based mobile computed tomography: a comparison with established imaging on the basis of simulated treatments of talus neck fractures in a cadaveric study. Comput Aided Surg. 2004;9:27–38. doi: 10.1080/10929080400006309. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
