

Surgical resection for persistent seroma, following modified radical mastectomy
- PMID: 17888182
- PMCID: PMC2082032
- DOI: 10.1186/1477-7819-5-104
Surgical resection for persistent seroma, following modified radical mastectomy
Abstract
Background: Seroma formation following modified radical mastectomy with axillary lymph node dissection for breast cancer is a most common wound complication. In our experience seroma occurs in approximately 50% of patients undergoing mastectomy. Postmastectomy seromas usually vanishes within a few weeks after operation.
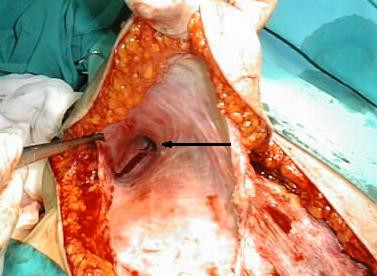
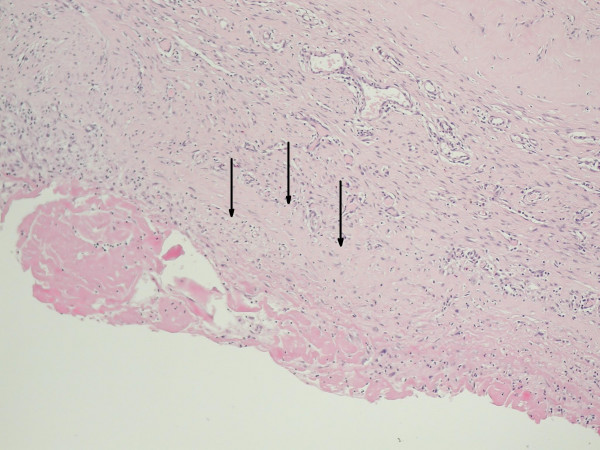
Case presentation: In this report we present the case of a 73 year old woman who had undergone mastectomy with axillary lymph node dissection for breast cancer, complicated by lymphorrhea and formation fibrous encapsulated seroma resistant to conservative treatment which required surgical resection.
Conclusion: We stand in opinion that in some cases of prolonged seromatous effusion with confirmed formation of thick walled reservoir the operation with resection and closure of supplying regional lymph vessels may be the best treatment, if possible preceded by arm lymphoscyntygraphy.
Figures
References
-
- Say CC, Donegan W. A biostatistical evaluation of complications from mastectomy. Surg Gynaecol Obstet. 1974;138:370–376. - PubMed
-
- Petrek JA, Peters MM, Nori S, Knauer C, Kinne DW, Rogatko A. Axillary lymphadenectomy. A prospective randomized trial of 13 factors influencing drainage including early or delayed arm mobilization. Arch Surg. 1990;125:378–382. - PubMed
-
- Kumar S, Lal B, Misra MC. Post-mastectomy seroma: a new look into the aetiology of an old problem. J R Coll Surg Edinb. 1995;40:292–294. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
