

High resolution Fourier-domain optical coherence tomography of retinal angiomatous proliferation
- PMID: 17891017
- PMCID: PMC2583219
- DOI: 10.1097/IAE.0b013e31805468fd
High resolution Fourier-domain optical coherence tomography of retinal angiomatous proliferation
Abstract
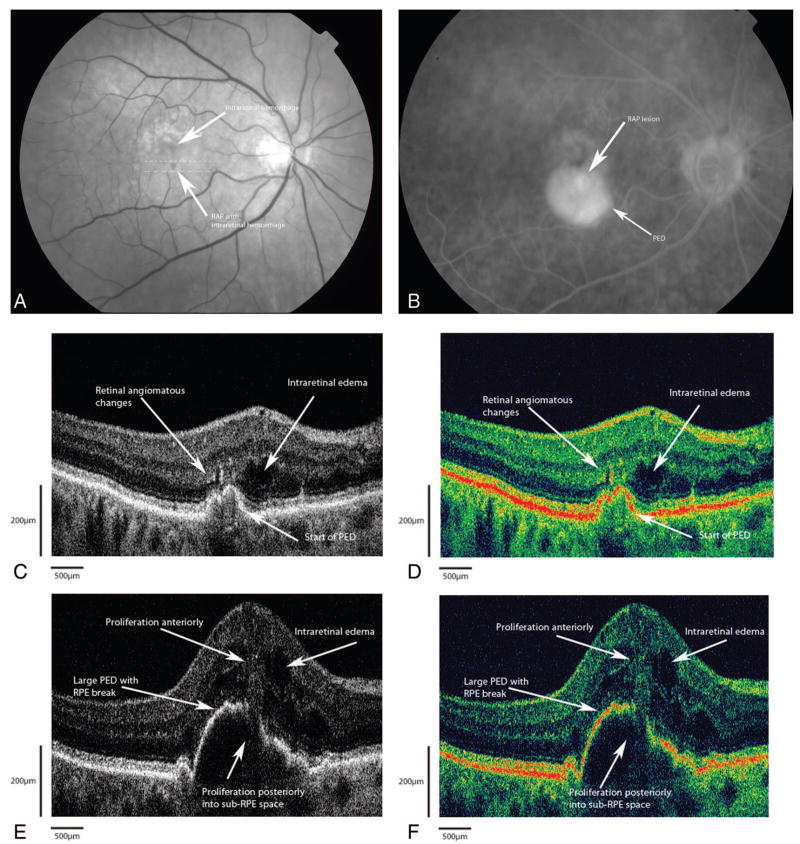
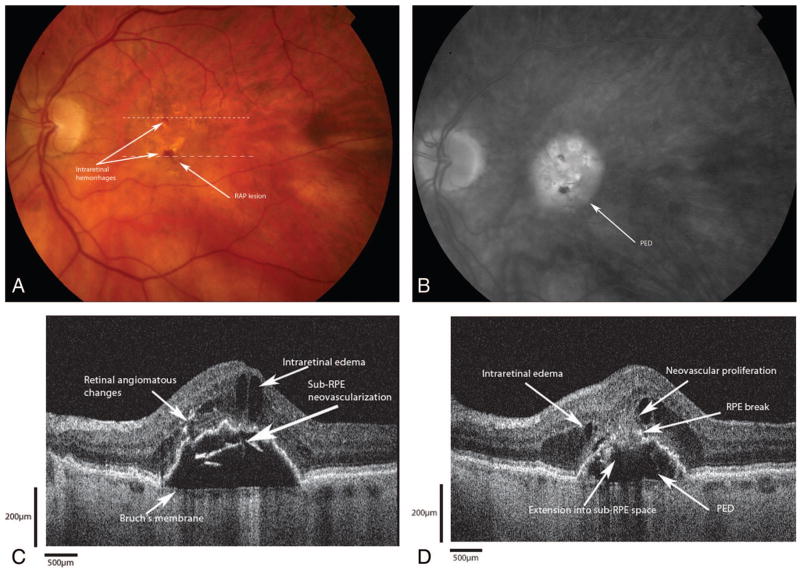
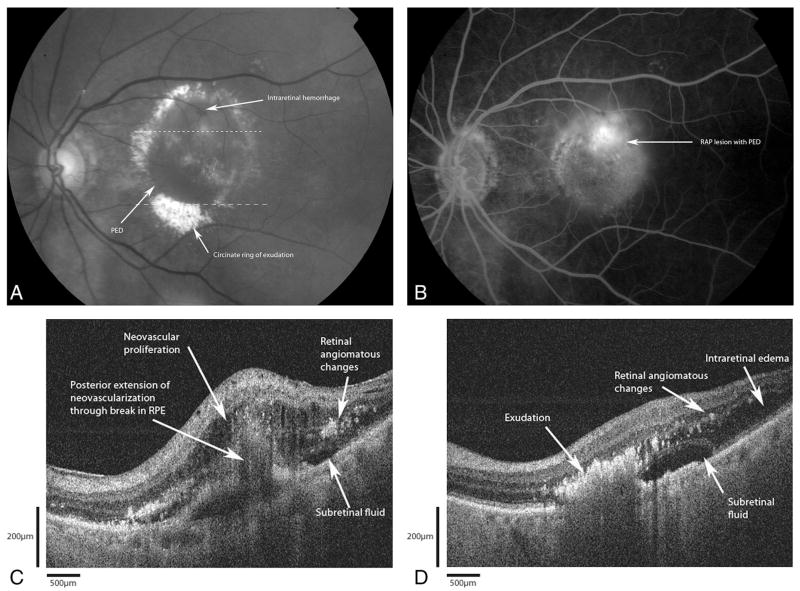
Purpose: To study the anatomic details of retinal angiomatous proliferation (RAP) in patients with age-related macular degeneration (AMD) using high-resolution Fourier-domain optical coherence tomography (Fd-OCT) and its three-dimensional reconstructions.
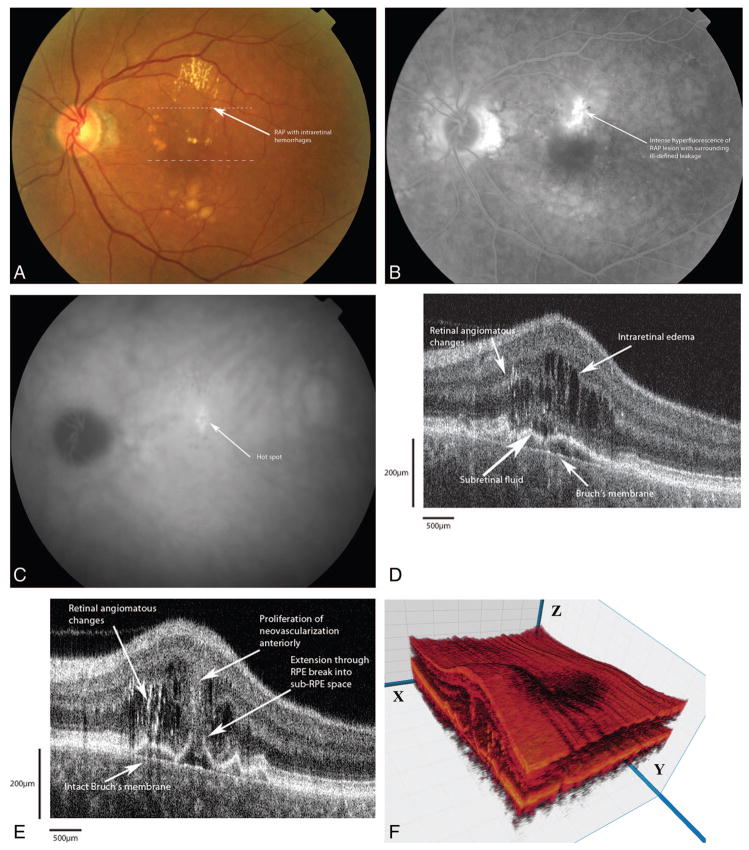
Methods: A Fd-OCT instrument was used to image five patients clinically diagnosed with RAP. A series of 100 raster-scanned B-scans centered over the macula was registered and rendered as a three-dimensional volume. These retinal structures were analyzed for anatomic details of the RAP lesions.
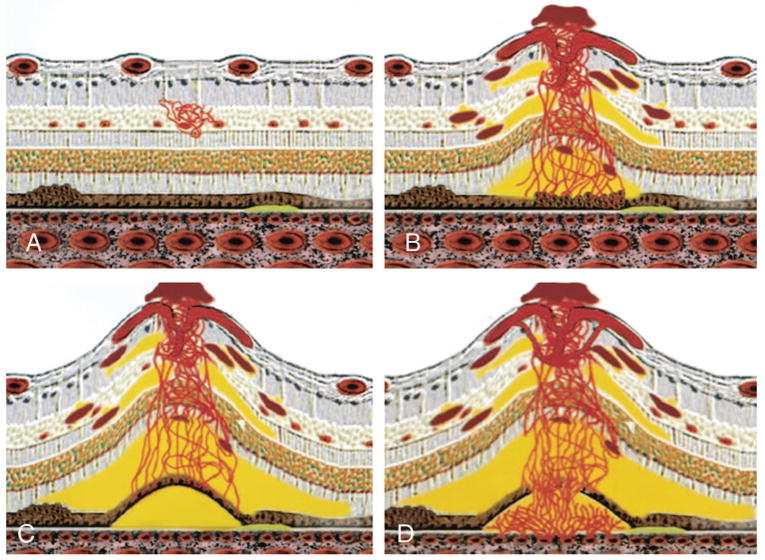
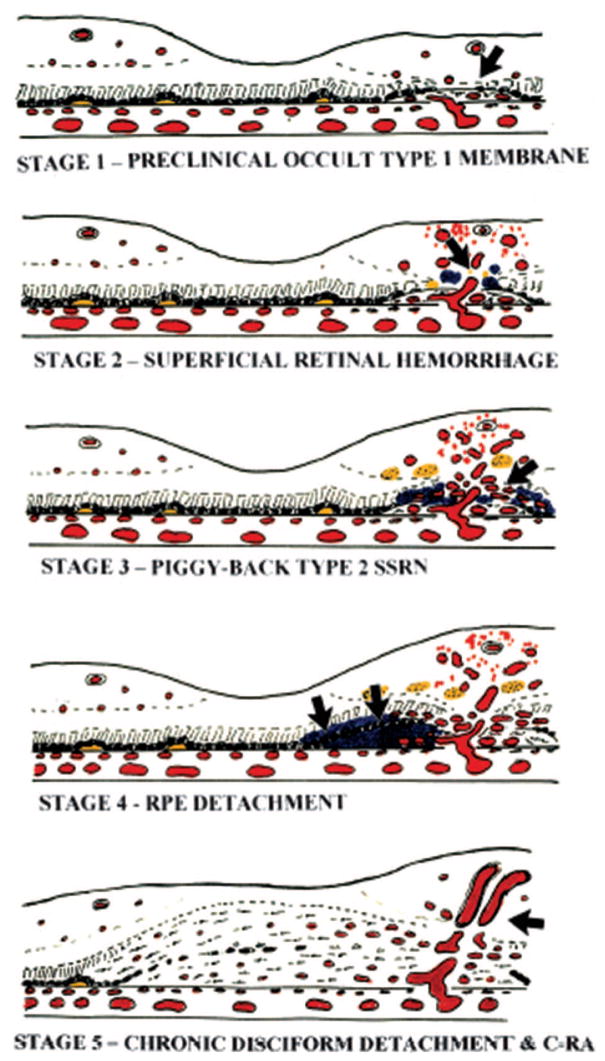
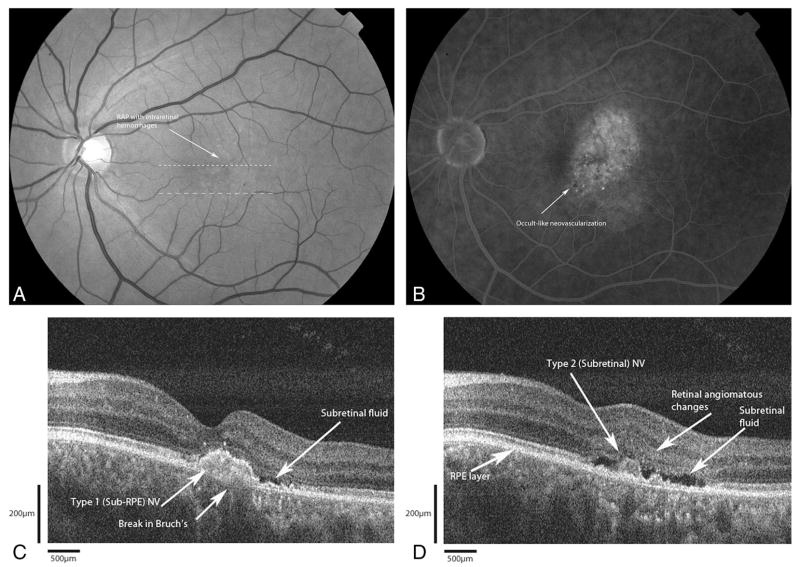
Results: The RAP lesion could be identified within the retina on Fd-OCT in all five cases. Fd-OCT images of the first four cases revealed areas of intraretinal neovascularization (IRN) in the deep retina adjacent to a pigment epithelial detachment (PED). There was neovascular proliferation anteriorly and posteriorly through a break in the retinal pigment epithelium (RPE). In three of the four cases, Bruch membrane remained intact. There was no identifiable choroidal neovascularization (CNV). The fifth case had both subretinal and sub-RPE neovascular membranes without a PED.
Conclusion: Fd-OCT provides unprecedented in vivo detail of the anatomy of RAP lesions that nearly resembles histologic specimens. This study suggests that the initial neovascular process in RAP can originate either within the retina or in the sub-RPE space.
Figures
References
-
- Freund KB, Klais CM, Eandi CM, et al. Sequenced combined intravitreal triamcinolone and indocyanine green angiography-guided photodynamic therapy for retinal angiomatous proliferation. Arch Ophthalmol. 2006;124:487–492. - PubMed
-
- Hartnett ME, Weiter JJ, Gardts A, Jalkh AE. Classification of retinal pigment epithelium detachments associated with drusen. Graefes Arch Clin Exp Ophthalmol. 1992;230:11–19. - PubMed
-
- Hartnett ME, Weiter JJ, Staurenghi G, Elsner AE. Deep retinal vascular anomalous complexes in advanced age-related macular degeneration. Ophthalmology. 1996;103:2042–2053. - PubMed
-
- Kuhn D, Meunier I, Soubrane G, Coscas G. Imaging of chorioretinal anastomoses in vascularized RPE detachments. Arch Ophthalmol. 1995;113:1392–1398. - PubMed
-
- Slakter JS, Yannuzzi LA, Schneider U, et al. Retinal choroidal anastomoses and occult choroidal neovascularization in age-related macular degeneration. Ophthalmology. 2000;107:742–754. - PubMed
