

Is a 3-mm intrafractional margin sufficient for daily image-guided intensity-modulated radiation therapy of prostate cancer?
- PMID: 17892900
- PMCID: PMC2759187
- DOI: 10.1016/j.radonc.2007.08.008
Is a 3-mm intrafractional margin sufficient for daily image-guided intensity-modulated radiation therapy of prostate cancer?
Abstract
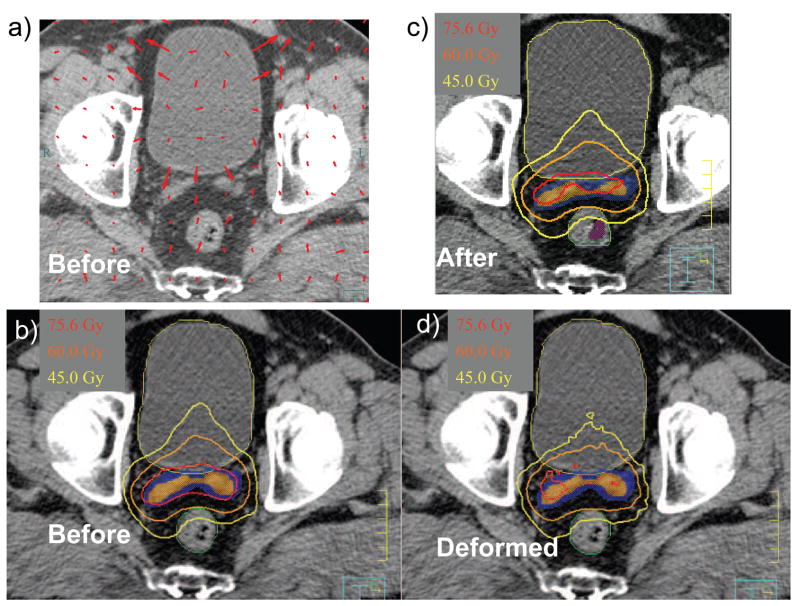
Purpose: To determine whether a 3-mm isotropic target margin adequately covers the prostate and seminal vesicles (SVs) during administration of an intensity-modulated radiation therapy (IMRT) treatment fraction, assuming that daily image-guided setup is performed just before each fraction.
Materials and methods: In-room computed tomographic (CT) scans were acquired immediately before and after a daily treatment fraction in 46 patients with prostate cancer. An eight-field IMRT plan was designed using the pre-fraction CT with a 3-mm margin and subsequently recalculated on the post-fraction CT. For convenience of comparison, dose plans were scaled to full course of treatment (75.6 Gy). Dose coverage was assessed on the post-treatment CT image set.
Results: During one treatment fraction (21.4+/-5.5 min), there were reductions in the volumes of the prostate and SVs receiving the prescribed dose (median reduction 0.1% and 1.0%, respectively, p<0.001) and in the minimum dose to 0.1 cm(3) of their volumes (median reduction 0.5 and 1.5 Gy, p<0.001). Of the 46 patients, three patients' prostates and eight patients' SVs did not maintain dose coverage above 70 Gy. Rectal filling correlated with decreased percentage-volume of SV receiving 75.6, 70, and 60 Gy (p<0.02).
Conclusions: The 3-mm intrafractional margin was adequate for prostate dose coverage. However, a significant subset of patients lost SV dose coverage. The rectal volume change significantly affected SV dose coverage. For advanced-stage prostate cancers, we recommend to use larger margins or improve organ immobilization (such as with a rectal balloon) to ensure SV coverage.
Conflict of interest statement
None of the authors have any actual or potential conflicts of interest.
Figures




References
-
- Ezzell GA, Galvin JM, Low D, et al. Guidance document on delivery, treatment planning, and clinical implementation of IMRT: report of the IMRT Subcommittee of the AAPM Radiation Therapy Committee. Med Phys. 2003;30:2089–2115. - PubMed
-
- Mohan R, Barest G, Brewster LJ, et al. A comprehensive three-dimensional radiation treatment planning system. Int J Radiat Oncol Biol Phys. 1988;15:481–495. - PubMed
-
- Purdy JA. Advances in three-dimensional treatment planning and conformal dose delivery. Semin Oncol. 1997;24:655–671. - PubMed
-
- Purdy JA. 3D treatment planning and intensity-modulated radiation therapy. Oncology (Williston Park) 1999;13:155–168. - PubMed
-
- McBain CA, Henry AM, Sykes J, et al. X-ray volumetric imaging in image-guided radiotherapy: The new standard in on-treatment imaging. Int J Radiat Oncol Biol Phys. 2006;64:625–634. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
