

Cardiac Certificate of Need regulations and the availability and use of revascularization services
- PMID: 17893007
- PMCID: PMC2084214
- DOI: 10.1016/j.ahj.2007.06.031
Cardiac Certificate of Need regulations and the availability and use of revascularization services
Abstract
Background: Many states enforce Certificate of Need (CON) regulations for cardiac procedures, but little is known about how CON affects utilization. We assessed the association between cardiac CON regulations, availability of revascularization facilities, and revascularization rates.
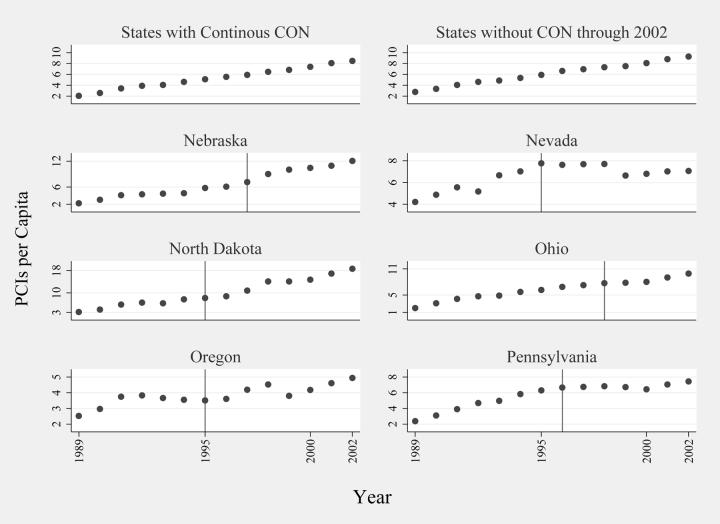
Methods: We determined when state cardiac CON regulations were active and obtained data for Medicare beneficiaries > or = 65 years old who received coronary artery bypass graft surgery (CABG) or a percutaneous coronary intervention (PCI) between 1989 and 2002. We compared the number of hospitals performing revascularization and patient utilization in states with and without CON regulations, and in states which discontinued CON regulations during 1989 to 2002.
Results: Each year, the per capita number of hospitals performing CABG and PCI was higher in states without CON (3.7 per 100,000 elderly for CABG, 4.5 for PCI in 2002), compared with CON states (2.5 for CABG, 3.0 for PCI in 2002). Multivariate regressions that adjusted for market and population characteristics found no difference in CABG utilization rates between states with and without CON (P = .7). However, CON was associated with 19.2% fewer PCIs per 1000 elderly (P = .01), equivalent to 322,526 fewer PCIs for 1989 to 2002. Among most states that discontinued CON, the number of hospitals performing PCI rose in the mid 1990s, but there were no consistent trends in the number of hospitals performing CABG or in PCIs or CABGs per capita.
Conclusions: Certificate of Need restricts the number of cardiac facilities, but its effect on utilization rates may vary by procedure.
Figures




References
-
- Nichols LM, Ginsburg PB, Berenson RA, Christianson J, Hurley RE. Are market forces strong enough to deliver efficient health care systems? Confidence is waning. Health Aff (Millwood ) 2004;23(2):8–21. - PubMed
-
- Enthoven AC. Market forces and efficient health care systems. Health Aff (Millwood ) 2004;23(2):25–27. - PubMed
-
- Popescu I, Vaughan-Sarrazin MS, Rosenthal GE. Certificate of Need regulations and use of coronary revascularization after acute myocardial infarction. JAMA. 2006;295(18):2141–2147. - PubMed
-
- Conover CJ, Sloan FA. Does removing Certificate-of-Need regulations lead to a surge in health care spending? Journal of Health Politics, Policy and Law. 1998;23(3):455–481. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
