

Diffusion tensor MR imaging tractography of the pyramidal tracts correlates with clinical motor function in children with congenital hemiparesis
- PMID: 17893220
- PMCID: PMC8134215
- DOI: 10.3174/ajnr.A0676
Diffusion tensor MR imaging tractography of the pyramidal tracts correlates with clinical motor function in children with congenital hemiparesis
Abstract
Background and purpose: Children with congenital hemiparesis have greater asymmetry in diffusion parameters of the pyramidal tracts compared with control subjects. We hypothesized that the asymmetry correlates with the severity of hemiparesis and that diffusion metrics would be abnormal in the affected tracts and normal in the unaffected tracts.
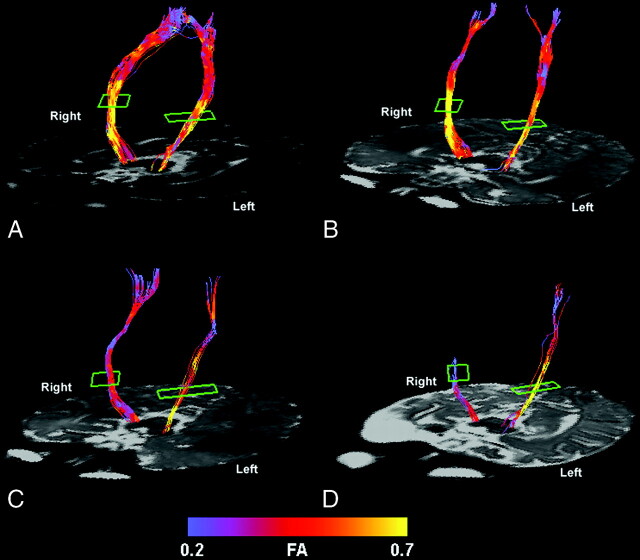
Materials and methods: Fifteen patients with congenital hemiparesis and 17 age-matched control subjects were studied with diffusion tensor MR imaging tractography. Hemipareses were scored as mild, moderate, or severe. We measured tract-specific diffusion parameters (fractional anisotropy, mean, and directional diffusion coefficients) of the pyramidal tracts. We compared tract-specific parameters and asymmetry between the right and left tracts of the differing severity groups and control subjects.
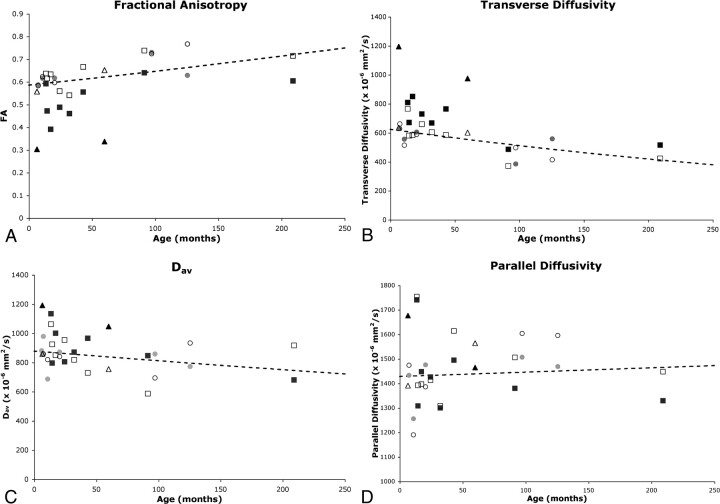
Results: We observed many different causes of congenital hemiparesis including venous infarction, arterial infarction, and polymicrogyria. Clinical severity of hemiparesis correlated with asymmetry in fractional anisotropy (P < .0001), transverse diffusivity (P < .0001), and mean diffusivity (P < .03). With increasing severity of hemiparesis, fractional anisotropy decreased (P < .0001) and transverse diffusivity (P < .0001) and mean diffusivity (P < .02) increased in the affected pyramidal tract compared with controls. Diffusion metrics in the unaffected tract were similar to those in the control subjects.
Conclusion: Asymmetry in fractional anisotropy, transverse diffusivity, and mean diffusivity, as well as the degree of abnormality in the actual values of the affected pyramidal tracts themselves, correlates with the severity of motor dysfunction in infants and children with congenital hemiparesis from different causes. This suggests that abnormalities detected by diffusion tensor MR imaging tractography in the affected pyramidal tract are related to the functional ability of the affected pyramidal tract, regardless of the etiology of motor dysfunction.
Figures
References
-
- Hagberg B, Hagberg G, Beckung E, et al. Changing panorama of cerebral palsy in Sweden. VIII. Prevalence and origin in the birth year period 1991–94. Acta Paediatr 2001;90:271–77 - PubMed
-
- Cioni G, Bartalena L, Biagioni E, et al. Neuroimaging and functional outcome of neonatal leukomalacia. Behav Brain Res 1992;49:7–19 - PubMed
-
- Humphreys P, Whiting S, Pham B. Hemiparetic cerebral palsy: clinical pattern and imaging in prediction of outcome. Can J Neurol Sci 2000;27:210–19 - PubMed
-
- Kotlarek F, Rodewig R, Brull D, et al. Computed tomographic findings in congenital hemiparesis in childhood and their relation to etiology and prognosis. Neuropediatrics 1981;12:101–09 - PubMed
-
- Molteni B, Oleari G, Fedrizzi E, et al. Relation between CT patterns, clinical findings and etiological factors in children born at term, affected by congenital hemiparesis. Neuropediatrics 1987;18:75–80 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical