

Use of protein antigens for early serological diagnosis of leprosy
- PMID: 17898185
- PMCID: PMC2168166
- DOI: 10.1128/CVI.00299-07
Use of protein antigens for early serological diagnosis of leprosy
Abstract
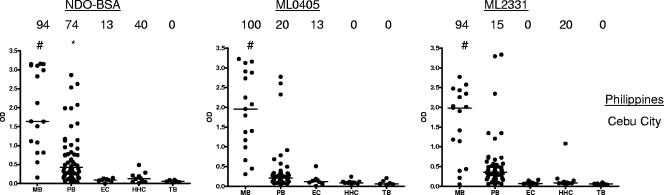
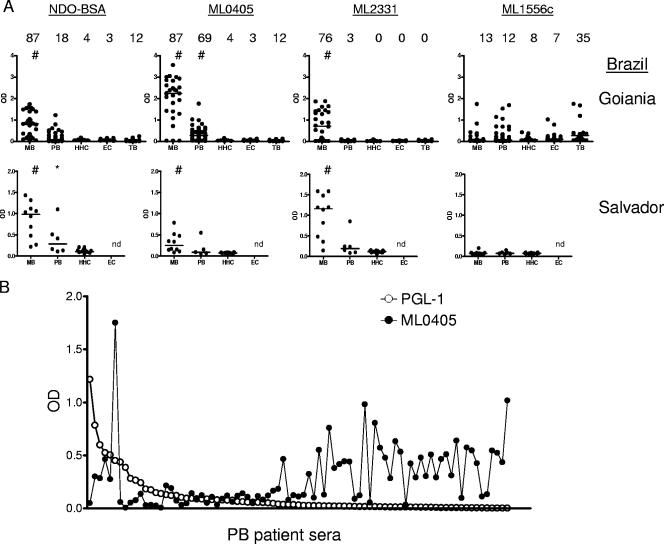
Leprosy is a chronic and debilitating human disease caused by infection with the Mycobacterium leprae bacillus. Despite the marked reduction in the number of registered worldwide leprosy cases as a result of the widespread use of multidrug therapy, the number of new cases detected each year remains relatively stable. This indicates that M. leprae is still being transmitted and that, without earlier diagnosis, M. leprae infection will continue to pose a health problem. Current diagnostic techniques, based on the appearance of clinical symptoms or of immunoglobulin M (IgM) antibodies that recognize the bacterial phenolic glycolipid I, are unable to reliably identify early-stage leprosy. In this study we examine the ability of IgG within leprosy patient sera to bind several M. leprae protein antigens. As expected, multibacillary leprosy patients provided stronger responses than paucibacillary leprosy patients. We demonstrate that the geographic locations of the patients can influence the antigens they recognize but that ML0405 and ML2331 are recognized by sera from diverse regions (the Philippines, coastal and central Brazil, and Japan). A fusion construct of these two proteins (designated leprosy IDRI diagnostic 1 [LID-1]) retained the diagnostic activity of the component antigens. Upon testing against a panel of prospective sera from individuals who developed leprosy, we determined that LID-1 was capable of diagnosing leprosy 6 to 8 months before the onset of clinical symptoms. A serological diagnostic test capable of identifying and allowing treatment of early-stage leprosy could reduce transmission, prevent functional disabilities and stigmatizing deformities, and facilitate leprosy eradication.
Figures




References
-
- Anderson, H., B. Stryjewska, B. L. Boyanton, and M. R. Schwartz. 2007. Hansen disease in the United States in the 21st century: a review of the literature. Arch. Pathol. Lab. Med. 131:982-986. - PubMed
-
- Bakker, M. I., M. Hatta, A. Kwenang, P. Van Mosseveld, W. R. Faber, P. R. Klatser, and L. Oskam. 2006. Risk factors for developing leprosy—a population-based cohort study in Indonesia. Lepr. Rev. 77:48-61. - PubMed
-
- Buhrer, S. S., H. L. Smits, G. C. Gussenhoven, C. W. van Ingen, and P. R. Klatser. 1998. A simple dipstick assay for the detection of antibodies to phenolic glycolipid-I of Mycobacterium leprae. Am. J. Trop. Med. Hyg. 58:133-136. - PubMed
-
- Buhrer-Sekula, S., H. L. Smits, G. C. Gussenhoven, J. van Leeuwen, S. Amador, T. Fujiwara, P. R. Klatser, and L. Oskam. 2003. Simple and fast lateral flow test for classification of leprosy patients and identification of contacts with high risk of developing leprosy. J. Clin. Microbiol. 41:1991-1995. - PMC - PubMed
-
- Cartel, J. L., S. Chanteau, J. P. Boutin, R. Plichart, P. Richez, J. F. Roux, and J. H. Grosset. 1990. Assessment of anti-phenolic glycolipid-I IgM levels using an ELISA for detection of M. leprae infection in populations of the South Pacific Islands. Int. J. Lepr. Other Mycobact. Dis. 58:512-517. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
