

Case Reports
doi: 10.3174/ajnr.A0717.
Epub 2007 Sep 26.
Marginal sinus arteriovenous fistulas mimicking carotid cavernous fistulas: diagnostic and therapeutic considerations
Affiliations
- PMID: 17898196
- PMCID: PMC8134241
- DOI: 10.3174/ajnr.A0717
Item in Clipboard
Case Reports
Marginal sinus arteriovenous fistulas mimicking carotid cavernous fistulas: diagnostic and therapeutic considerations
AJNR Am J Neuroradiol.
2007 Nov-Dec.
Abstract
Marginal sinus fistulas (MSFs) are uncommon vascular anomalies. Occasionally, the dominant venous drainage is forced retrograde up the inferior petrosal sinus and into the cavernous sinus, causing chemosis, proptosis, and ocular hypertension, mimicking a carotid cavernous fistula. This atypical clinical presentation may lead to misdiagnosis and inappropriate hazardous treatment of an MSF. Identifying the site of the fistula and understanding the anatomy of the venous drainage are critical in providing appropriate, safe, and efficacious endovascular treatment.
Figures
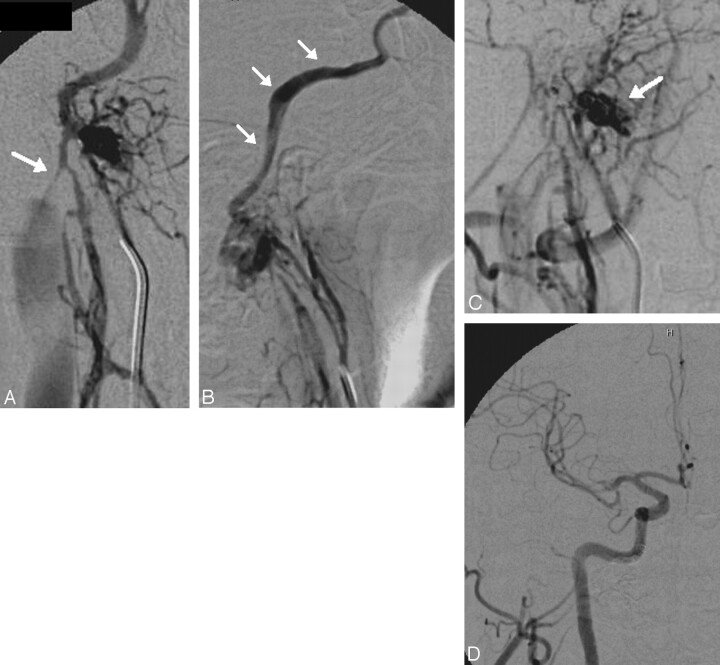
A 45-year-old man with a right marginal sinus DAVF. Posteroanterior (PA) (A) and lateral projections (B) from a right ascending pharyngeal angiogram demonstrate an arteriovenous fistula supplied by numerous branches of the neuromeningeal trunk with dominant outflow retrograde (B, white arrows) into the IPS, CS, and ultimately the SOV, accounting for a clinical presentation indistinguishable from a CCF. Antegrade outflow via the ipsilateral jugular vein is limited by a high-grade flow-related stenosis at the skull base (A, white arrow). Access into the recipient pouch was achieved via a transfemoral transjugular approach. However, during the process of coil embolization, the microcatheter was kicked out of the recipient pouch and could not be navigated back in, to complete the occlusion of the fistula. C, Superselective angiogram from a catheter positioned within a neuromeningeal branch of the ascending pharyngeal artery demonstrates persistent filling of the recipient pouch (arrow) following partial coil embolization. For this reason, the embolization was completed with a transarterial-to-venous infusion of Onyx-18. D, Control angiography in the PA projection demonstrates complete ablation of the fistula with no residual arteriovenous shunt surgery.
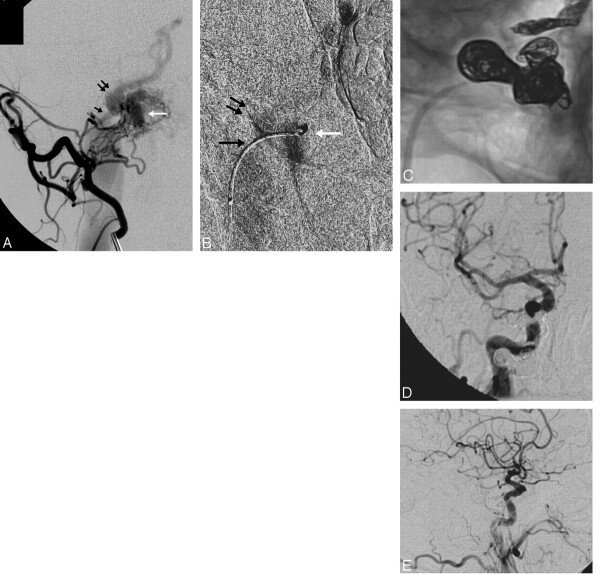
A 67-year-old man with progressive proptosis, chemosis, headache, and pulse synchronous bruit. A, Oblique view from a selective injection of the right occipital artery demonstrates arteriovenous shunt surgery into a marginal sinus recipient pouch (white arrow). Antegrade drainage into the ipsilateral jugular vein is limited by a high-grade stenosis at the junction of the pouch and the IJ vein (black arrow). The dominant venous drainage is via a patulous connection with the IPS (double arrow), which is proximally dilated and flows out into the CS and SOV. A microcatheter was successfully navigated into the fistulous pouch. B, Selective venography performed from a microcatheter positioned within the recipient venous pouch (white arrow) confirms the anatomy of the pouch and its venous outflow through the stenotic channel into the IJ vein (black arrow) and retrograde up the IPS (double arrows). The introduction of coils into the pouch resulted in instability of the microcatheter, which was repeatedly pushed back into the proximal IPS. For this reason, the IPS was coil-occluded to stabilize the microcatheter within the pouch. After this was performed, additional coils were introduced into the recipient pouch, resulting in complete occlusion of the fistula. C, Native oblique view demonstrates coils distributed within the right IPS and marginal sinus recipient pouch. Common carotid angiography in the PA (D) and lateral (E) projections demonstrate complete occlusion of the fistula, with no residual arteriovenous shunt surgery. Following the procedure, the patient's symptoms completely resolved.
References
-
- De Oliveira E, Rhoton AL, Peace D. Microsurgical anatomy of the region of the foramen magnum. Surg Neurol 1985;24:293–352 - PubMed
-
- Awad IA, Little JR, Akrawi WP, et al. Intracranial dural arteriovenous malformations: factors predisposing to an aggressive neurological course. J Neurosurg 1990;72:839–50 - PubMed
-
- Brown RD, Wiebers DO, Nichols DA. Intracranial dural arteriovenous fistulae: angiographic predictors of intracranial hemorrhage and clinical outcome in nonsurgical patients. J Neurosurg 1994;81:531–38 - PubMed
-
- Djindjian R, Merland JJ. Super-Selective Arteriography of the External Carotid Artery. New York: Springer-Verlag;1978
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous