

Sixty-four-row multisection CT angiography for detection and evaluation of ruptured intracranial aneurysms: interobserver and intertechnique reproducibility
- PMID: 17898200
- PMCID: PMC8134231
- DOI: 10.3174/ajnr.A0699
Sixty-four-row multisection CT angiography for detection and evaluation of ruptured intracranial aneurysms: interobserver and intertechnique reproducibility
Abstract
Background and purpose: The purpose of this work was to assess intertechnique and interobserver reproducibility of 64-row multisection CT angiography (CTA) used to detect and evaluate intracranial aneurysms.
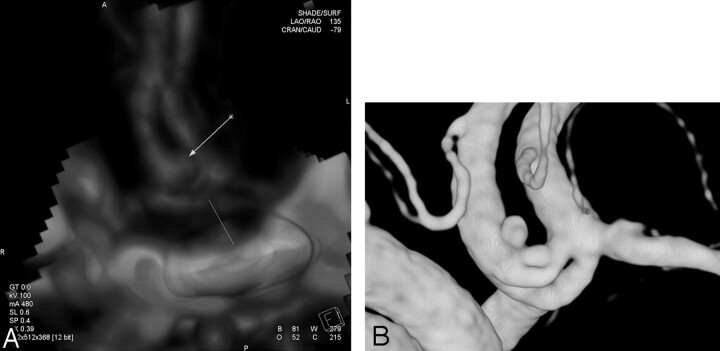
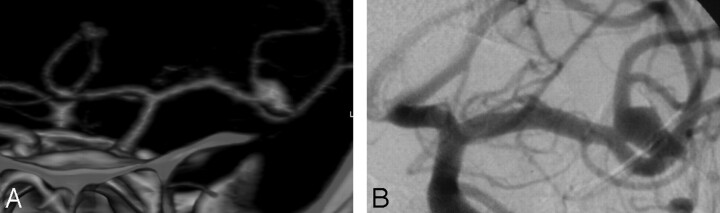
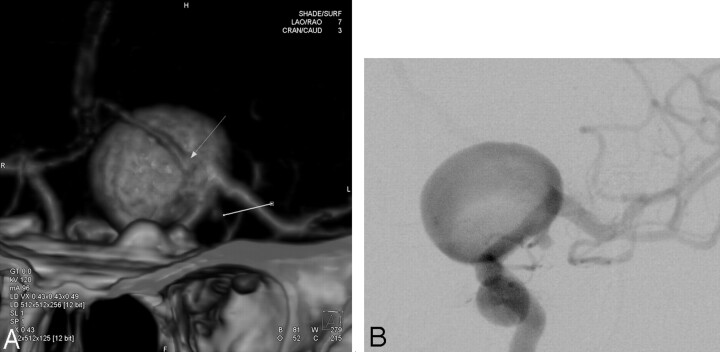
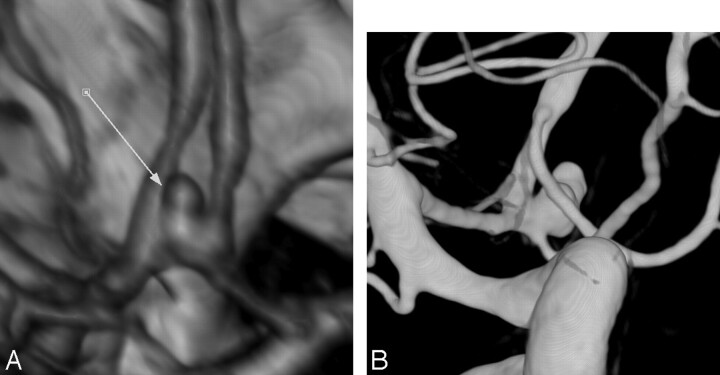
Materials and methods: From October 2005 to November 2006, 54 consecutive patients with nontraumatic subarachnoid hemorrhage (SAH) underwent both CTA and digital substraction angiography (DSA). Four radiologists independently reviewed CT images, and 2 other radiologists reviewed DSA images. Aneurysm diameter (D), neck width (N), and the presence of a branch arising from the sac were assessed.
Results: DSA revealed 67 aneurysms in 48 patients and no aneurysm in 6 patients. Mean sensitivity and specificity of CTA for the detection of intracranial aneurysms were, respectively, 94% and 90.2%. For aneurysms less than 3 mm, CTA had a mean sensitivity of 70.4%. Intertechnique and interobserver agreements were good for the detection of aneurysms (mean kappa = 0.673 and 0.732, respectively) and for the measurement of their necks (mean kappa = 0.753 and 0.779, respectively). Intertechnique and interobserver agreements were excellent for the measurement of aneurysm diameters (mean kappa = 0.847 and 0.876, respectively). In addition, CTA was accurate in determining the N/D ratio of aneurysms and adjacent arterial branches. However, the N/D ratio was overestimated by all of the readers at CTA.
Conclusion: Sixty-four-row multisection CTA is an imaging method with a good interobserver reproducibility and a high sensitivity and specificity for the detection and the morphologic evaluation of ruptured intracranial aneurysms. It may be used as an alternative to DSA as a first-intention imaging technique in patients with SAH.
Figures
Comment in
-
CT angiography is state-of-the-art first vascular imaging for subarachnoid hemorrhage.AJNR Am J Neuroradiol. 2008 Jun;29(6):e41-2; author reply e46-7. doi: 10.3174/ajnr.A1049. Epub 2008 Mar 27. AJNR Am J Neuroradiol. 2008. PMID: 18372411 Free PMC article. No abstract available.
References
-
- Linn FH, Rinkel GJ, Algra A, et al. Incidence of subarachnoid hemorrhage: role of region year and rate of CT scanning: a meta-analysis. Stroke 1996;27:625–29 - PubMed
-
- Mayberg MR, Batjer HH, Dacey, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke 1994;25:2315–28 - PubMed
-
- Cloft HJ, Joseph GJ, Dion JE. Risk of cerebral angiography in patients with subarachnoid hemorrhage, cerebral aneurysms, and arteriovenous malformations: a meta-analysis. Stroke 1999;30:317–20 - PubMed
-
- Schwartz RB, Tice HM, Hooten SM, et al. Evaluation of cerebral aneurysms with helical CT: correlation with conventional angiography and MR angiography. Radiology 1994;192:717–22 - PubMed
-
- Liang EY, Chan M, Hsiang JH, et al. Detection and assessment of intracranial aneurysms: value of CT angiography with shaded-surface display. AJR Am J Roentgenol 1995;165:1497–502 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical