

What is new in iron overload?
- PMID: 17899187
- PMCID: PMC2254659
- DOI: 10.1007/s00431-007-0604-y
What is new in iron overload?
Abstract
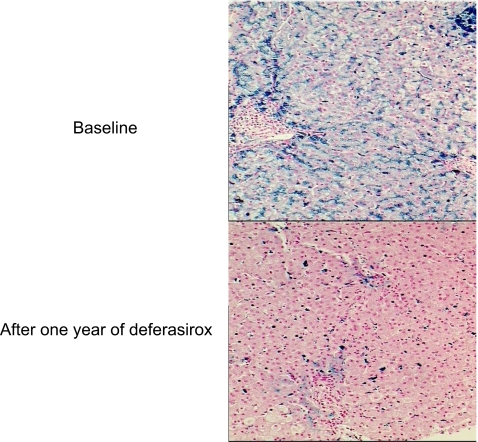
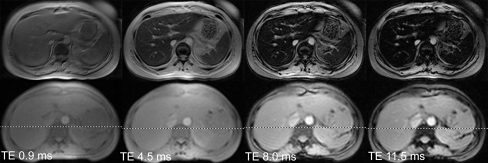
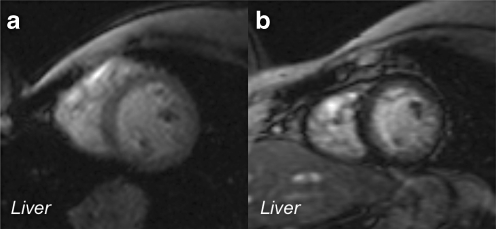
Children with severe chronic hemolytic anemia or congenital erythroblastopenia are transfusion dependent. Long-term transfusion therapy prolongs life but results in a toxic accumulation of iron in the organs. The human body cannot actively eliminate excess iron. Therefore, the use of a chelating agent is required to promote excretion of iron. So far, iron chelation has been done by subcutaneous infusion of deferoxamine given over 10 h, 5-6 days per week. Compliance is poor and chelation often insufficient. Ferritin measurements and sometimes liver biopsies are used to evaluate the iron burden in the body. At the present time, new iron chelators that can be given orally are available. Furthermore, magnetic resonance imaging (MRI) assessment of tissue iron is a noninvasive and highly reproducible method, which is able to quantitate organ iron burden. In conclusion, iron overload can be measured more accurately with noninvasive methods such as MRI. Deferasirox is a once-daily oral therapy for treating transfusional iron overload, which improves patient compliance and quality of life.
Figures
References
-
- Cappellini MD, Cohen A, Piga A, Bejaoui M, Perrotta S, Agaoglu L, Aydinok Y, Kattamis A, Kilinc Y, Porter J, Capra M, Galanello R, Fattoum S, Drelichman G, Magnano C, Verissimo M, Athanassiou-Metaxa M, Giardina P, Kourakli-Symeonidis A, Janka-Schaub G, Coates T, Vermylen C, Olivieri N, Thuret I, Opitz H, Ressayre-Djaffer C, Marks P, Alberti D (2006) A phase 3 study of deferasirox (ICL670), a once daily oral iron chelator, in patients with beta thalassemia. Blood 107:3455–3462 - DOI - PubMed
-
- Cohen AR (2006) New advances in iron chelation therapy. http://www.asheducationbook.org Hematology 2006 42–47 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
