

Screw fixation via diploic bone paralleling to occiput table: anatomical analysis of a new technique and report of 11 cases
- PMID: 17899218
- PMCID: PMC2140140
- DOI: 10.1007/s00586-007-0500-1
Screw fixation via diploic bone paralleling to occiput table: anatomical analysis of a new technique and report of 11 cases
Abstract
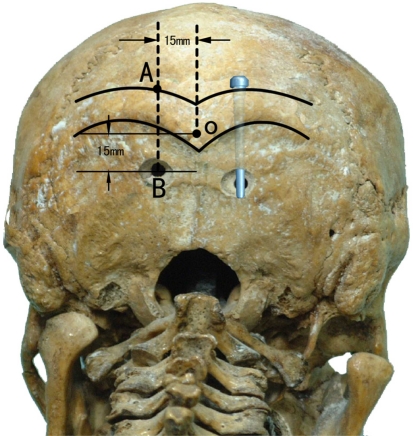
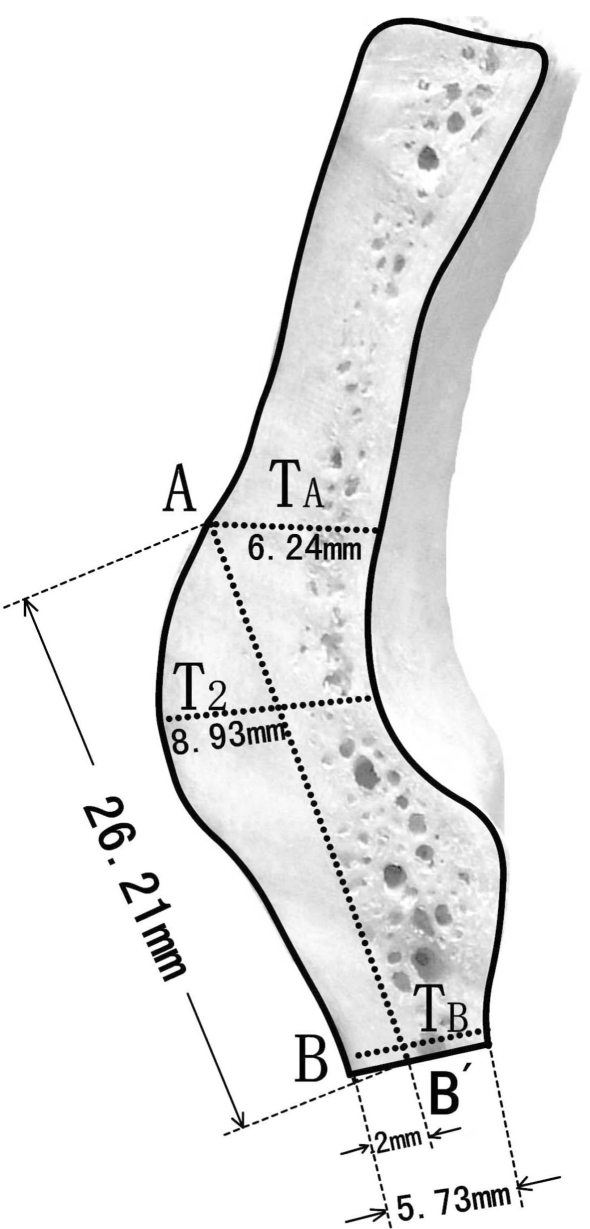
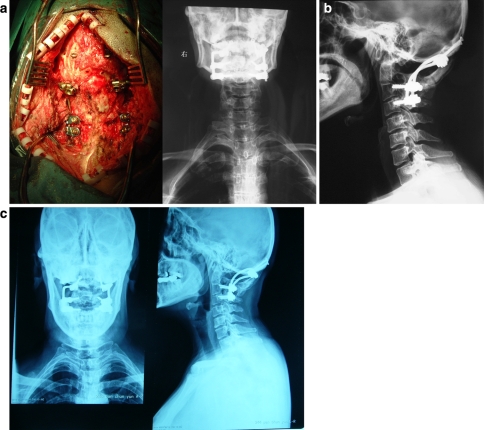
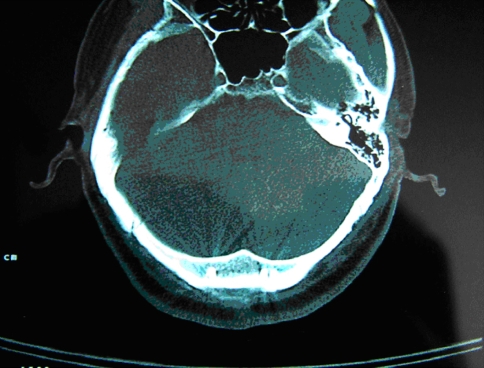
Several types of posterior approaches have been adopted for occipitocervical fusion. Prior to this study, Foerater et al. in 1927 used a fibular strut graft in the site between the occiput and the lower cervical spine to achieve fusion. Since then, various techniques including wrings, Hartshill loop, AO reconstructive plate, and AXIS occipital plate were described and used widely. As far as we know, all these techniques involve the screw placement vertical to the diploic bone; however none has ever addressed the feasibility of screw placement in occiput parallelling to the diploic bone. In our study, 30 dry specimens of human occiputs were measured manually using vernier calipers and protractors. The intradiploic screw was first supposed to be inserted inferiorly to the superior nuchal line (SNL) prominence. The entry point located at the superior edge of the SNL prominence. Afterward, the measurements of extracranial occiput in SNL area on midline and bilateral 15 mm to the midline saggital-cutting planes of the occiput were conducted. The thickness of the occipital bone at the location of SNL prominence, the entry point, the exit point and the screw orientation were measured, respectively. Afterward, 11 patients with craniocervical malformation were treated surgically using this alternative and their X-ray radiographs and CT scans were evaluated postoperatively. The data showed that the occipital at the site of SNL prominence was the thickest. The thickest point was external occipital protuberance (EOP), which was up to 14 mm. The thickness decreased gradually from the site of SNL to the superior border of surgical decompressed area. The actual length of screw channel was about 26 mm. The mean thickness for safe screw insertion ranged from 5.73 to 14.14 mm. A total of 22 intraocciput screws parallel to diploic bone were placed precisely, without injury to the cerebral and inner occipital venous sinus. The results confirm that occiput is available for holding intraocciput screw paralleling to diploic bone.
Figures

References
-
- Abumi K, Ito H, Taneichi H, Kaneda K (1994) Transpedicular screw fixation for traumatic lesions of the middle and lower cervical spine: description of the techniques and preliminary report. Spinal Disord 7:19–28 - PubMed
-
- Bridwell KH, DeWald RL (1997) The textbook of spinal surgery. Lippincott-Raven, Philadelphia, pp 986–990
-
- Doherty BJ, Esses SI, Heggeness MH (1991) A biomechanical study of occipital–cervical fixation. Presented at the Cervical Spine Research Society. Philadelphia, Pennsylvania
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
