

Audit of deaths less than a week after admission through an emergency department: how accurate was the ED diagnosis and were any deaths preventable?
- PMID: 17901266
- PMCID: PMC2658432
- DOI: 10.1136/emj.2006.044867
Audit of deaths less than a week after admission through an emergency department: how accurate was the ED diagnosis and were any deaths preventable?
Abstract
Aim: To review the causes of death in patients admitted via the emergency department (ED) who died within 7 days of admission and to identify any ways in which ED care could have been better. The study also aims to compare the diagnosis made in the ED and the mortality diagnosis.
Methods: A retrospective study; subjects were all patients who attended the ED over 4 months and died within 7 days of admission. The paramedics' notes, ED case cards, inpatient medical notes and details of postmortem findings were examined to identify the time and date of arrival in the ED, presenting complaint, provisional diagnosis made by the ED, treatment plan devised by the ED, diagnosis made in wards, and the cause of death as issued on death certificates or from postmortem findings. Summary sheets of cases where the care provided by the emergency department could have been improved were reviewed, errors were identified and deaths were classified as preventable or unpreventable.
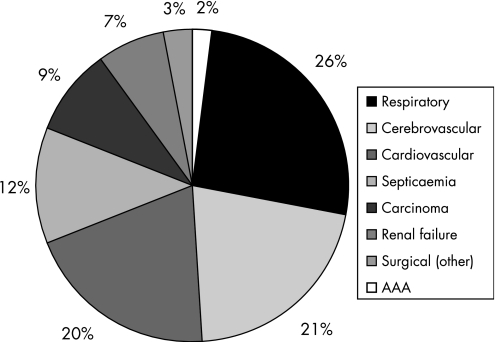
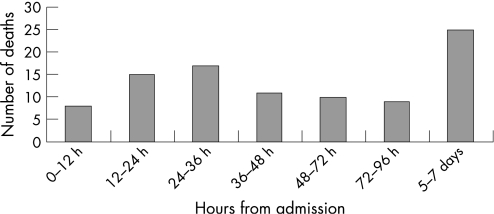
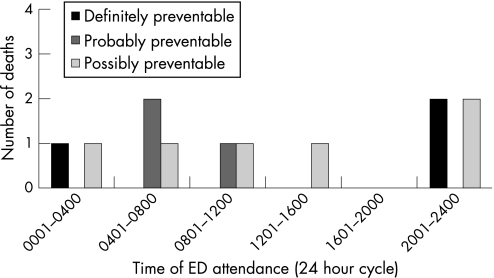
Results: Database revealed 3521 admissions via the ED over 4 months, of which 95 cases (2.69%) died within 7 days of admission. 78 patients (82.1% of cases) were appropriately diagnosed and managed whereas 17 (17.87% of cases) were identified with deficiencies in either the diagnosis or the management provided in the ED. We reviewed the quality of care provided in the ED for these cases and rated deaths according to our preventability criteria: 5 (5.26%) deaths were unpreventable despite the deficiency in care provided in the ED; 3 (3.15%) deaths were definitely preventable; 3 (3.15%) were probably preventable; and 6 (6.31%) were possibly preventable deaths.
Conclusion: The ED is playing a good role in the management of critically ill patients, with appropriate diagnosis and management in 82% of cases. Training of junior doctors is required to prevent occurrence of errors and thus preventable deaths, but all deaths are not preventable. New guidelines for sepsis management and management of undifferentiated clinical presentations are being introduced and we intend to audit the implications of new guidelines.
Conflict of interest statement
Competing interests: None.
Similar articles
-
Unexpected death within 72 hours of emergency department visit: were those deaths preventable?Crit Care. 2015 Apr 8;19(1):154. doi: 10.1186/s13054-015-0877-x. Crit Care. 2015. PMID: 25887707 Free PMC article.
-
Who is less likely to die in association with improved National Emergency Access Target (NEAT) compliance for emergency admissions in a tertiary referral hospital?Aust Health Rev. 2016 Apr;40(2):149-154. doi: 10.1071/AH14242. Aust Health Rev. 2016. PMID: 26278814
-
Preventable deaths in patients admitted from emergency department.Emerg Med J. 2006 Jun;23(6):452-5. doi: 10.1136/emj.2004.022319. Emerg Med J. 2006. PMID: 16714507 Free PMC article.
-
Causes of death among non-urgent patients in the emergency department who die within 30 days.Dan Med J. 2023 Sep 25;70(10):A01230037. Dan Med J. 2023. PMID: 37897388 Review.
-
The national review of asthma deaths: what did we learn and what needs to change?Breathe (Sheff). 2015 Mar;11(1):14-24. doi: 10.1183/20734735.008914. Breathe (Sheff). 2015. PMID: 26306100 Free PMC article. Review.
Cited by
-
The death of diagnosis.Clin Med (Lond). 2012 Jun;12(3):301-2. doi: 10.7861/clinmedicine.12-3-301. Clin Med (Lond). 2012. PMID: 22783793 Free PMC article. No abstract available.
-
Emergency Department Deaths in a Nigerian University Hospital: Deaths Too Many.West Indian Med J. 2015 Mar;64(2):131-4. doi: 10.7727/wimj.2013.281. Epub 2015 Mar 13. West Indian Med J. 2015. PMID: 26360686 Free PMC article.
-
Red-flag sepsis and SOFA identifies different patient population at risk of sepsis-related deaths on the general ward.Medicine (Baltimore). 2018 Dec;97(49):e13238. doi: 10.1097/MD.0000000000013238. Medicine (Baltimore). 2018. PMID: 30544383 Free PMC article.
-
Prehospital triage of patients diagnosed with perforated peptic ulcer or peptic ulcer bleeding: an observational study of patients calling 1-1-2.Scand J Trauma Resusc Emerg Med. 2018 Apr 5;26(1):25. doi: 10.1186/s13049-018-0494-1. Scand J Trauma Resusc Emerg Med. 2018. PMID: 29618372 Free PMC article.
-
Emergency department patient safety incident characterization: an observational analysis of the findings of a standardized peer review process.BMC Emerg Med. 2014 Aug 8;14:20. doi: 10.1186/1471-227X-14-20. BMC Emerg Med. 2014. PMID: 25106803 Free PMC article.
References
-
- Arnstein F. Catalogue of human error. Br J Anaesth 199779645–656. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources