

Economic evaluation of a rehabilitation program integrating exercise, self-management, and active coping strategies for chronic knee pain
- PMID: 17907207
- PMCID: PMC2675012
- DOI: 10.1002/art.23011
Economic evaluation of a rehabilitation program integrating exercise, self-management, and active coping strategies for chronic knee pain
Abstract
Objective: To conduct an economic evaluation of the Enabling Self-Management and Coping with Arthritic Knee Pain through Exercise (ESCAPE-knee pain) program.
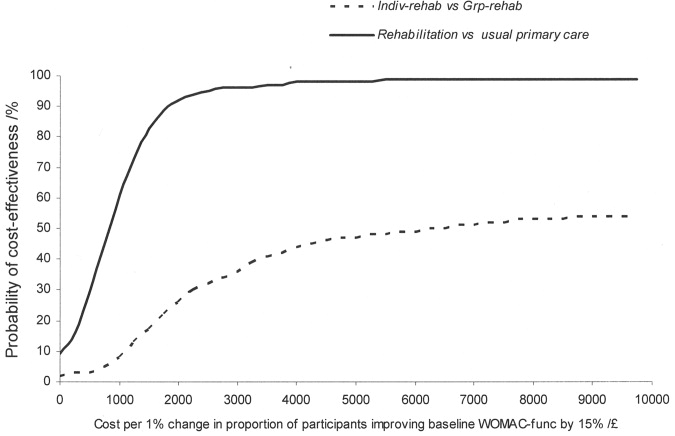
Methods: Alongside a clinical trial, we estimated the costs of usual primary care and participation in ESCAPE-knee pain delivered to individuals (Indiv-rehab) or groups of 8 participants (Grp-rehab). Information on resource use and informal care received was collected during face-to-face interviews. Cost-effectiveness and cost-utility were assessed from between-group differences in costs, function (primary clinical outcome), and quality-adjusted life years (QALYs). Cost-effectiveness acceptability curves were constructed to represent uncertainty around cost-effectiveness.
Results: Rehabilitation (regardless of whether Indiv-rehab or Grp-rehab) cost 224 pounds (95% confidence interval [95% CI] 184 pounds, 262 pounds) more per person than usual primary care. The probability of rehabilitation being more cost-effective than usual primary care was 90% if decision makers were willing to pay 1,900 pounds for improvements in functioning. Indiv-rehab cost 314 pounds/person and Grp-rehab 125 pounds/person. Indiv-rehab cost 189 pounds (95% CI 168 pounds, 208 pounds) more per person than Grp-rehab. The probability of Indiv-rehab being more cost-effective than Grp-rehab increased as willingness to pay (WTP) increased, reaching 50% probability at WTP 5,500 pounds. The lack of differences in QALYs across the arms led to lower probabilities of cost-effectiveness based on this outcome.
Conclusion: Provision of ESCAPE-knee pain had small cost implications, but it was more likely to be cost-effective in improving function than usual primary care. Group rehabilitation reduces costs without compromising clinical effectiveness, increasing probability of cost-effectiveness.
Figures

References
-
- Badley EM, Rasooly I, Webster GK. Relative importance of musculoskeletal disorders as a cause of chronic health problems, disability, and health care utilization: findings from the 1990 Ontario Health Survey. J Rheumatol. 1994;21:505–14. - PubMed
-
- Badley EM, Ibanez D. Socioeconomic risk factors and musculoskeletal disability. J Rheumatol. 1994;21:515–22. - PubMed
-
- Dawson J, Linsell L, Zondervan K, Rose P, Randall T, Carr A, et al. Epidemiology of hip and knee pain and its impact on overall health status in older adults. Rheumatology (Oxford) 2004;43:497–504. - PubMed
-
- Alonso J, Ferrer M, Gandek B, Ware JE, Aaronson NK, Mosconi P, IQOLA Project Group et al. Health-related quality of life associated with chronic conditions in eight countries: results from the International Quality of Life Assessment (IQOLA) Project. Qual Life Res. 2004;13:283–98. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
